
Application of electronic laryngoscope combined with narrow band imaging endoscope and its classification in the diagnosis of vocal cord leukoplakia
-
摘要: 目的 探讨电子喉镜结合窄带成像(narrow band imaging,NBI)内镜及其分型在声带白斑诊断中的临床应用价值。 方法 回顾性分析2020年9月至2022年11月在南京鼓楼医院门诊就诊,经过电子喉镜和NBI内镜检查,初步诊断为声带白斑,并且均在门诊进行活检,送病理检查的患者资料115例,研究声带白斑的形态特征和NBI分型与病理结果之间的相关性。 结果 115例初诊为声带白斑的患者中,病理结果诊断为良性病变46例(40.00%),低度上皮内瘤变29例(25.22%),高度上皮内瘤变(包括原位癌)22例(19.13%),浸润癌(包括可疑浸润癌)18例(15.65%)。声带白斑的单双侧与病理结果的分布差异无统计学意义(P>0.05),声带白斑的大小、厚薄、病变是否均匀、边界是否清晰、是否侵犯前联合、是否对称、年龄是否大于55岁、形态分型、NBI分型与病理结果分布均差异有统计学意义(P<0.05)。形态分型(平坦型、隆起型、粗糙型)3组间两两比较,仅平坦型和粗糙型比较P<0.017,其他2组间比较均P>0.017。NBI分型(Ⅲ、Ⅳ、Ⅴ)的3组间两两比较,均差异有统计学意义(P<0.017)。NBI分型与病理诊断有较高的相关性,相关系数为0.705(P<0.05)。NBI内镜的Ⅳ型为高度上皮内瘤变及癌变的风险是Ⅲ型的9.125倍,Ⅴ型为高度上皮内瘤变及癌变的风险是Ⅲ型的271.078倍。形态分型和NBI分型的曲线下面积分别为0.672和0.896。 结论 NBI分型与病理诊断之间有较高的匹配度和关联性,电子喉镜结合NBI内镜对声带白斑有较高的诊断价值,对恶性白斑有较强的预判能力。Abstract: Objective To investigate the clinical value of electronic laryngoscope combined with narrow band imaging(NBI) endoscope and its classification in the diagnosis of vocal cord leukoplakia. Methods A retrospective analysis was performed on 115 cases of patients treated in the Department of Otolaryngology, Head and Neck Surgery, Nanjing Drum Tower Hospital from September 2020 to November 2022. All 115 cases were diagnosed with vocal cord leukogramma using the electronic laryngoscopy and narrow band imaging endoscopy, followed by pathological examination in the outpatient tissue biopsy. The morphological characteristics of vocal cord leukoplakia and the correlation between narrow band imaging classification and pathological results were investigated. Results Among 115 cases of vocal cord leukoplakia, 46 cases(40.00%) were diagnosed as benign lesions. Low grade intraepithelial neoplasia occurred in 29 cases(25.22%). High-grade intraepithelial neoplasia(including carcinoma in situ) occurred in 22 cases(19.13%). Invasive carcinoma(including suspected invasive carcinoma) was found in 18 cases(15.65%). There were no statistical differences in the unilateral and bilateral distribution of vocal cord leukoplakia and pathological results(P>0.05), but there were statistical differences in the size, thickness, lesion uniformity, clear boundary, pre-invasion commissure, symmetry, age over 55 years old, morphological classification, NBI classification and pathological results distribution(P < 0.05). The two-by-two comparison among the three groups of morphological classification(flat type, raised type, rough type) showed that P < 0.017 was only compared between flat type and rough type, and P>0.017 was compared between the other two groups. The pairwise comparison among the three groups of NBI classification(Ⅲ, Ⅳ, Ⅴ) was statistically significant(P < 0.017). There was a high correlation between NBI classification and pathological diagnosis, and the correlation coefficient was 0.705(P < 0.05). The risk of high intraepithelial neoplasia and cancerization in type Ⅳ was 9.125 times higher than that in type Ⅲ, and the risk of high intraepithelial neoplasia and cancerization in type Ⅴ was 271.078 times higher than that in type Ⅲ. The area under the curve of morphological classification and NBI classification were 0.672 and 0.896, respectively. Conclusion There is a high match and correlation between NBI classification and pathological diagnosis. Electronic laryngoscope combined with narrow band imaging endoscope has a high diagnostic value for vocal cord leukoplakia, and a strong predictive ability for malignant leukoplakia.
-

-
表 1 电子喉镜和NBI内镜下声带白斑不同特征的病理类型分布
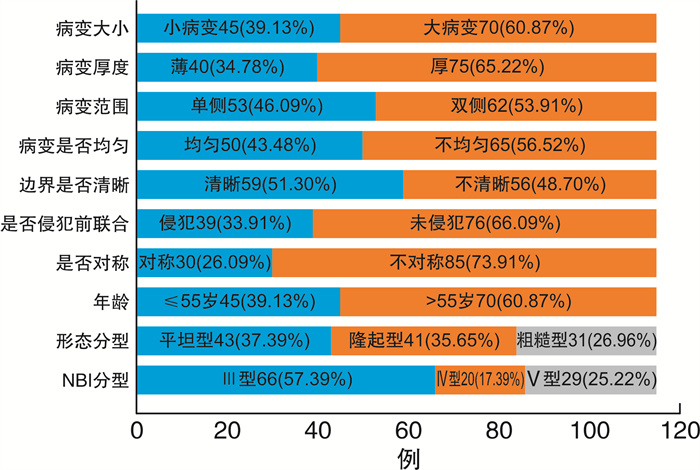
病变特征 总例数(n=115) 良性病变(n=46) 低度上皮内瘤变(n=29) 高度上皮内瘤变(n=22) 癌变(n=18) Z或H P 病变大小 -4.532 <0.001 小(<50%) 45 29(64.40) 9(20.00) 6(13.30) 1(2.20) 大(≥50%) 70 17(24.30) 20(28.60) 16(22.90) 17(24.30) 病变厚度 -4.711 <0.001 薄 40 27(67.50) 8(20.00) 5(12.50) 0(0) 厚 75 19(25.30) 21(28.00) 17(22.70) 18(24.00) 病变范围 -0.244 0.807 单侧 53 21(39.62) 12(22.64) 12(22.64) 8(15.09) 双侧 62 25(40.32) 17(27.42) 10(16.13) 10(16.13) 病变是否均匀 -5.260 <0.001 是 50 33(66.00) 10(20.00) 6(12.00) 1(2.00) 否 65 13(20.00) 19(29.20) 16(24.60) 17(26.20) 边界是否清晰 -4.122 <0.001 是 59 32(54.20) 16(27.10) 9(15.30) 2(3.40) 否 56 14(25.00) 13(23.20) 13(23.20) 16(28.60) 是否侵犯前联合 -2.361 0.018 是 39 10(25.60) 11(28.20) 9(23.10) 9(23.10) 否 76 36(47.40) 18(23.70) 13(17.10) 9(11.80) 对称性 -2.395 0.017 是 30 19(63.30) 3(10.00) 5(16.70) 3(10.00) 否 85 27(31.80) 26(30.60) 17(20.00) 15(17.60) 年龄 -3.381 0.001 ≤55岁 45 27(60.00) 8(17.78) 7(15.56) 3(6.67) >55岁 70 19(27.14) 21(30.00) 15(21.43) 15(21.43) 形态学分型 17.707 <0.001 平坦 43 26(60.50) 9(20.90) 6(14.00) 2(4.70) 隆起 41 15(36.60) 11(26.80) 9(22.00) 6(14.60) 粗糙 31 5(16.10) 9(29.00) 7(22.60) 10(32.30) NBI分型 57.142 <0.001 Ⅲ 66 41(62.10) 20(30.30) 4(6.10) 1(1.50) Ⅳ 20 4(20.00) 8(40.00) 4(20.00) 4(20.00) Ⅴ 29 1(3.40) 1(3.40) 14(48.30) 13(44.80)  下载: 导出CSV
下载: 导出CSV
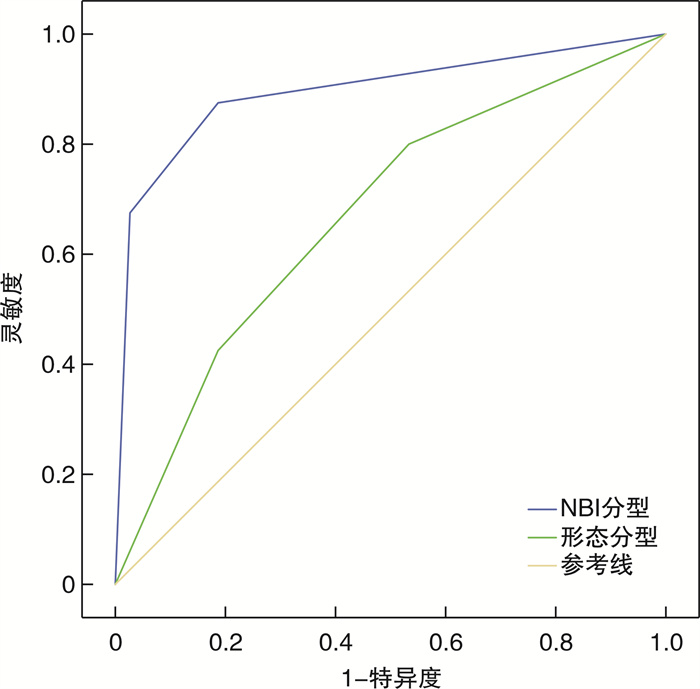
表 2 ROC曲线下面积
检验结果变量 曲线下面积 标准误差 P 95%CI 下限 上限 形态分型 0.672 0.053 0.002 0.569 0.775 NBI分型 0.896 0.036 <0.001 0.825 0.966
下载: 导出CSV
-
[1] 王琦, 黄杨熠艺, 李林荣, 等. 高清智能染色内镜结合频闪喉镜对声带白斑的诊疗价值[J]. 中华耳鼻咽喉头颈外科杂志, 2022, 57(7): 868-873. doi: 10.3760/cma.j.cn115330-20211021-00678
[2] 张宝根, 倪晓光. 窄带成像内镜对声带白斑诊断作用的研究进展[J]. 临床耳鼻咽喉头颈外科杂志, 2019, 33(11): 1113-1116. https://lceh.whuhzzs.com/article/doi/10.13201/j.issn.1001-1781.2019.11.027
[3] 张宝根, 倪晓光. 窄带成像内镜在头颈部肿瘤诊断中的应用[J]. 癌症进展, 2019, 17(2): 125-127, 161.
[4] 郑重, 万光伦, 陈浩, 等. 声带白斑的喉镜特征与病理相关性分析[J]. 听力学及言语疾病杂志, 2020, 28(3): 239-242. doi: 10.3969/j.issn.1006-7299.2020.03.001
[5] Ni XG, He S, Xu ZG, et al. Endoscopic diagnosis of laryngeal cancer and precancerous lesions by narrow band imaging[J]. J Laryngol Otol, 2011, 125(3): 288-296. doi: 10.1017/S0022215110002033
[6] El-Naggar AK, Chan JK, Grandis JR, et al. WHO classification of tumors of head and neck tumours[M]. 4th ed. Lyon: IARC Press, 2017: 77-104.
[7] 方三高. WHO(2017)头颈部肿瘤分类[J]. 诊断病理学杂志, 2017, 24(8): 638-641. doi: 10.3969/j.issn.1007-8096.2017.08.024
[8] 方三高, 魏建国, 周晓军. WHO(2017)头颈部肿瘤(下咽、喉、气管及咽旁间隙肿瘤)分类解读[J]. 临床与实验病理学杂志, 2019, 35(3): 308-311.
[9] 陈东辉, 郑宏良, 肖水芳, 等. 喉白斑诊断与治疗专家共识解读[J]. 中华耳鼻咽喉头颈外科杂志, 2018, 53(8): 570-574. doi: 10.3760/cma.j.issn.1673-0860.2018.08.003
[10] 王文伦, 张立红, 曹杰, 等. 声带白斑的发病因素及临床特点分析[J]. 中华耳鼻咽喉头颈外科杂志, 2018, 53(8): 581-586. doi: 10.3760/cma.j.issn.1673-0860.2018.08.005
[11] Rutt AL, Wang C, Li Z. Clinicopathologic aspects of vocal fold leukoplakia in smokers and nonsmokers[J]. J Voice, 2021, 35(5): 779-784. doi: 10.1016/j.jvoice.2020.02.003
[12] 李雯, 谭韵, 关力谦, 等. 窄带成像对声带白斑病变性质的预测研究[J]. 临床耳鼻咽喉头颈外科杂志, 2020, 34(5): 459-462. https://lceh.whuhzzs.com/article/doi/10.13201/j.issn.2096-7993.2020.05.018
[13] Lu GW, Guo WT, Zhang Q, et al. Endoscopic diagnosis value of narrow band imaging Ni classification in vocal fold leukoplakia and early glottic cancer[J]. Am J Otolaryngol, 2021, 42(3): 102904. doi: 10.1016/j.amjoto.2021.102904
[14] 张宝根, 倪晓光. 窄带成像内镜对声带白斑诊断作用的研究进展[J]. 临床耳鼻咽喉头颈外科杂志, 2019, 33(11): 1113-1116. https://lceh.whuhzzs.com/article/doi/10.13201/j.issn.1001-1781.2019.11.027
[15] Fang Y, Yang Y, Chen M, et al. Correlating intraepithelial papillary capillary loops of vocal cord leukoplakia with histopathology[J]. Acta Otolaryngol, 2022, 142(1): 106-111. doi: 10.1080/00016489.2021.2019828
[16] Leduchowska A, Morawska J, Pietruszewska W. Videolaryngoendoscopic and stroboscopic evaluation in predicting the malignancy risk of vocal fold leukoplakia[J]. J Clin Med, 2022, 11(19): 5789. doi: 10.3390/jcm11195789
[17] Chen M, Li CJ, Yang Y, et al. A morphological classification for vocal fold leukoplakia[J]. Braz J Otorhinolaryngol, 2019, 85(5): 588-596. doi: 10.1016/j.bjorl.2018.04.014
[18] Li LJ, Yu Z, Zhu JQ, et al. Laryngoscopic characteristics related to the risk of cancerization of vocal cord leukoplakia[J]. Acta Otolaryngol, 2021, 141(8): 802-807. doi: 10.1080/00016489.2021.1951444
[19] Ni XG, Zhu JQ, Zhang QQ, et al. Diagnosis of vocal cord leukoplakia: The role of a novel narrow band imaging endoscopic classification[J]. Laryngoscope, 2019, 129(2): 429-434. doi: 10.1002/lary.27346
[20] Lin CY, Zhang SS, Lu L, et al. Diagnostic value and pathological correlation of narrow band imaging classification in laryngeal lesions[J]. Ear Nose Throat J, 2021, 100(10): 737-741. doi: 10.1177/0145561320925327
-
图(3)
表(2)
计量
- 文章访问数: 487
- PDF下载数: 119
- 施引文献: 0