
-
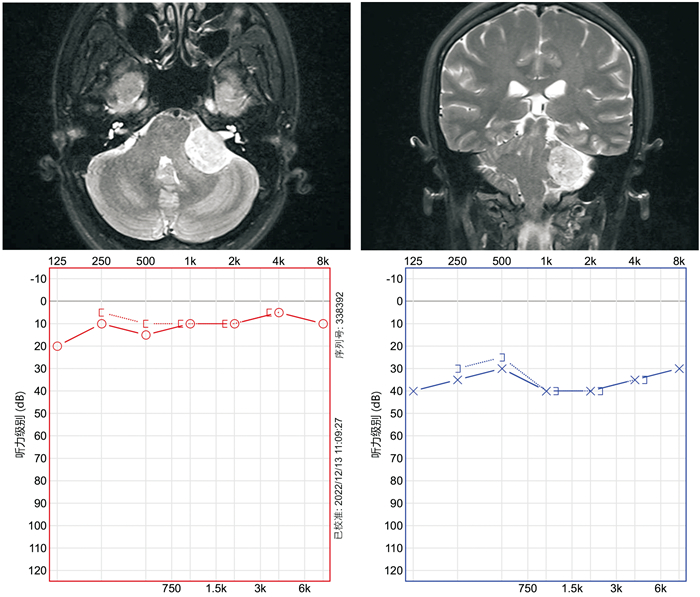
摘要: 目的 本研究旨在分析单侧听神经瘤患者的听力和前庭功能测试结果,并探讨其与肿瘤大小之间的关系。方法 回顾性分析完成纯音听力测试(PTA)、颈性和眼性前庭肌源诱发电位(c/oVEMP)、视频头脉冲测试(vHIT)且经手术治疗的81例单侧听神经瘤患者的临床资料。根据增强MRI上肿瘤最大径将患者分为小肿瘤组(≤15 mm)、中等大小肿瘤组(16~30 mm)和大肿瘤组(>30 mm)。结果 PTA测试结果显示,73例(90.1%)患者出现听力受损;前庭功能测试结果显示,前半规管、水平半规管、后半规管、椭圆囊、球囊异常率分别为29.6%、77.8%、54.3%、90.1%和92.6%。经统计学分析,不同分组患者术前听力测试结果差异无统计学意义(F=0.393,P=0.676),但水平半规管增益值(r=-0.248,P=0.025),水平半规管扫视波异常率(r=0.507,P<0.001),cVEMP阈值(χ2=15.111,P=0.004)以及oVEMP阈值(χ2=18.948,P<0.001)在不同大小肿瘤组之间差异有统计学意义。结论 听神经瘤患者的听力损失程度与肿瘤大小无关,但前庭功能的受损程度与肿瘤大小存在相关性。Abstract: Objective This study aimed to analyze the results of auditory and vestibular function tests in patients with unilateral vestibular schwannoma and explore their association with tumor size.Methods Clinical data from 81 patients diagnosed with unilateral vestibular schwannoma who underwent pure-tone audiometry(PTA), cervical and ocular vestibular evoked myogenic potentials(c/oVEMP), as well as video head impulse test(vHIT), and subsequently underwent surgical treatment, were retrospectively analyzed. Patients were categorized into groups based on tumor size: small (≤ 15 mm), medium(16-30 mm), and large (>30 mm), determined by the maximum tumor diameter on contrast-enhanced MRI scans.Results PTA results indicated hearing loss in 73 cases(90.1%); vestibular function tests revealed abnormal rates for the anterior semicircular canal, horizontal semicircular canal, posterior semicircular canal, utricle, and saccule at 29.6%, 77.8%, 54.3%, 90.1%, and 92.6%, respectively. Statistically, no significant differences were found in preoperative hearing test results among patients in different groups(F=0.393, P=0.676). However, significant differences were observed in horizontal semicircular canal gain(r=-0.248, P=0.025), abnormal rates of horizontal semicircular canal catch-up saccades(r=0.507, P < 0.001), as well as cVEMP(χ2=15.111, P=0.004) and oVEMP thresholds(χ2=18.948, P < 0.001) across varying tumor size groups.Conclusion The extent of hearing loss in patients with vestibular schwannoma is not correlated with tumor size, whereas the degree of vestibular dysfunction demonstrates a correlation with tumor size.
-

-
表 1 不同分组听神经瘤患者人口统计学、主诉及术前听力的比较
基本资料 小肿瘤组
(n=20)中等大小肿瘤组
(n=41)大肿瘤组
(n=20)合计
(n=81)F/χ2/H P 年龄/岁 42.6±12.5 50.1±11.5 48.8±12.5 47.9±12.3 2.716 0.072 性别/例(%) 1.090 0.580 女 14(70.0) 23(56.1) 12(60.0) 49(60.5) 男 6(30.0) 18(43.9) 8(40.0) 32(39.5) 侧别/例(%) 0.314 0.855 左 11(55.0) 20(48.8) 11(55.0) 42(51.9) 右 9(45.0) 21(51.2) 9(45.0) 39(48.1) 主诉/例(%) 听力下降 19(95.0) 39(95.1) 18(90.0) 76(93.8) 0.672 0.715 耳鸣 19(95.0) 35(85.4) 16(80.0) 70(86.4) 1.996 0.369 头晕/眩晕 9(45.0) 18(43.9) 8(40.0) 35(43.2) 0.118 0.943 头痛 3(15.0) 7(17.1) 6(30.0) 16(19.8) 1.796 0.407 面部麻木/疼痛 1(5.0) 6(14.6) 4(20.0) 11(13.6) 1.996 0.369 耳闷 3(15.0) 6(14.6) 2(10.0) 11(13.6) 0.292 0.864 舌头麻木/味觉减退 0(0) 4(9.8) 2(10.0) 6(7.4) 2.126 0.345 听力下降 19(95.0) 39(95.1) 18(90.0) 76(93.8) 0.672 0.715 病程/年 1.0(0.3~2.0) 2.0(0.5~4.0) 2.0(1.0~5.5) 2.0(0.6~3.0) 4.779 0.092 术前PTA/dB 57.1±33.3 59.7±27.5 65.5±35.5 60.5±30.8 0.393 0.676  下载: 导出CSV
下载: 导出CSV
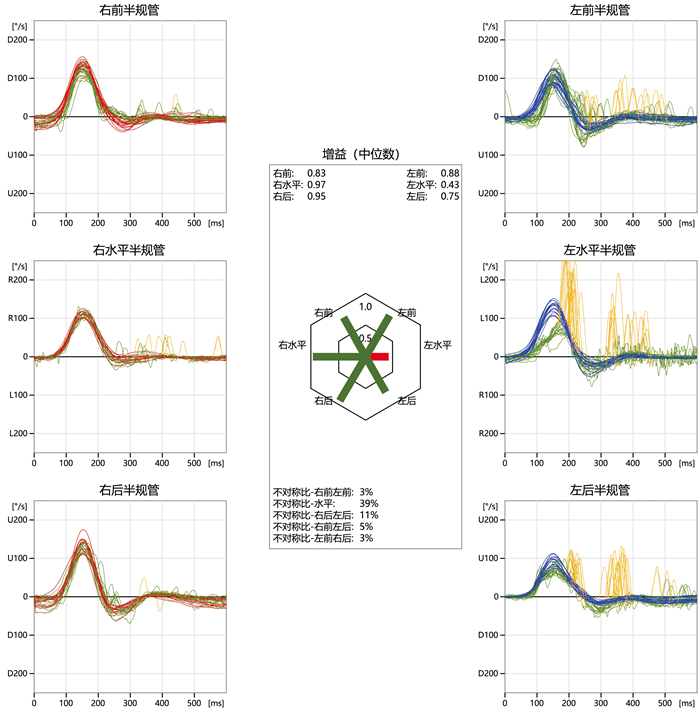
表 2 不同分组听神经瘤患者vHIT测试结果的比较
例(%) vHIT 小肿瘤组
(n=20)中等大小肿瘤组
(n=41)大肿瘤组
(n=20)合计
(n=81)F/χ2 P 前半规管 平均增益值 0.94±0.19 0.91±0.21 0.94±0.24 0.93±0.21 0.233 0.792 增益值异常 2(10.0) 8(19.5) 4(20.0) 14(17.3) 0.988 0.610 扫视波 4(20.0) 12(29.3) 8(40.0) 24(29.6) 1.924 0.382 水平半规管 平均增益值 0.80±0.31 0.74±0.20 0.62±0.14 0.72±0.23 3.357 0.040 增益值异常 5(25.0) 23(56.1) 18(90.0) 46(56.8) 17.234 < 0.001 扫视波 8(40.0) 35(85.4) 20(100.0) 63(77.8) 23.594 < 0.001 后半规管 平均增益值 0.92±0.14 0.84±0.21 0.82±0.20 0.86±0.20 1.569 0.215 增益值异常 1(5.0) 10(24.4) 6(30.0) 17(21.0) 4.349 0.114 扫视波 6(30.0) 27(65.9) 11(55.0) 44(54.3) 6.969 0.031
下载: 导出CSV
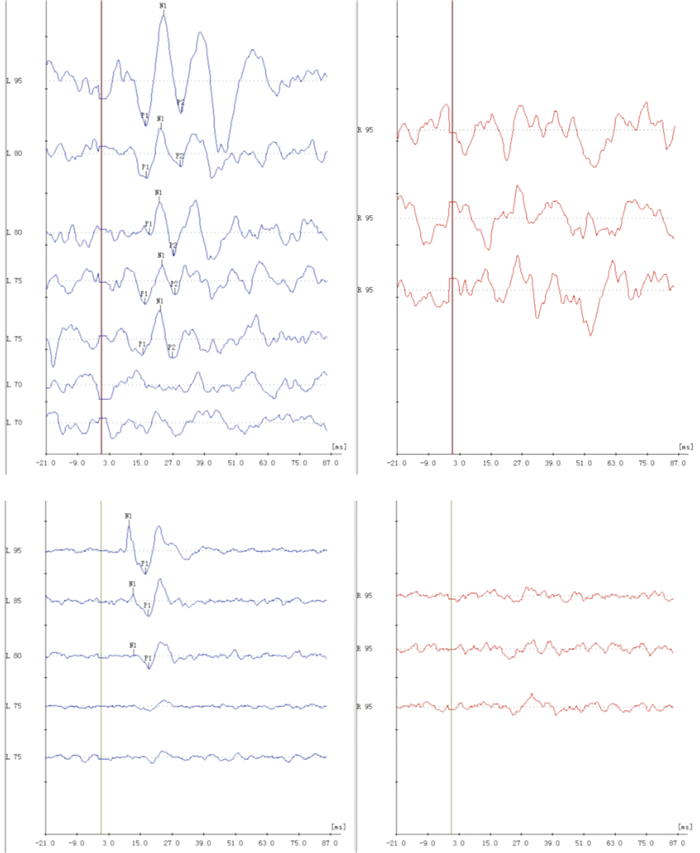
表 3 不同分组听神经瘤患者VEMP测试阈值的比较
例(%) VEMP阈值 小肿瘤组
(n=20)中等大小肿瘤组
(n=41)大肿瘤组
(n=20)合计
(n=81)χ2 P cVEMP 15.111 0.004 阈值正常 4(20.0) 3(7.3) 0(0) 7(8.6) 阈值升高 8(40.0) 8(19.5) 1(5.0) 17(21.0) 无反应 8(40.0) 30(73.2) 19(95.0) 57(70.4) oVEMP 18.948 0.001 阈值正常 5(25.0) 3(7.3) 0(0) 8(9.9) 阈值升高 5(25.0) 2(4.9) 0(0) 7(8.6) 无反应 10(50.0) 36(87.8) 20(100.0) 66(81.5)
下载: 导出CSV
表 4 不同分组听神经瘤患者cVEMP振幅不对称比的比较
例(%) cVEMP振幅不对称比 小肿瘤组
(n=18)中等大小肿瘤组
(n=36)大肿瘤组
(n=15)合计
(n=69)χ2 P 正常 < |±27%| 7(38.9) 4(11.1) 0(0) 11(15.9) 12.235 0.016 振幅减弱≥ 27% 10(55.6) 30(83.3) 15(100.0) 55(79.7) 振幅增强≥ 27% 1(5.6) 2(5.6) 0(0) 3(4.3)
下载: 导出CSV
表 5 不同分组听神经瘤患者oVEMP振幅不对称比的比较
例(%) oVEMP振幅不对称比 小肿瘤组
(n=18)中等大小肿瘤组
(n=35)大肿瘤组
(n=13)合计
(n=66)χ2 P 正常 < |±27%| 5(27.8) 0(0) 0(0) 5(7.6) 20.881 < 0.001 振幅减弱≥ 27% 11(61.1) 35(100.0) 13(100.0) 59(89.4) 振幅增强≥ 27% 2(11.1) 0(0) 0(0) 2(3.0)
下载: 导出CSV
-
[1] Carlson ML, Link MJ. Vestibular Schwannomas[J]. N Engl J Med, 2021, 384(14): 1335-1348. doi: 10.1056/NEJMra2020394
[2] Marinelli JP, Beeler CJ, Carlson ML, et al. Global Incidence of Sporadic Vestibular Schwannoma: A Systematic Review[J]. Otolaryngol Head Neck Surg, 2022, 167(2): 209-214. doi: 10.1177/01945998211042006
[3] von Kirschbaum C, Gürkov R. Audiovestibular Function Deficits in Vestibular Schwannoma[J]. Biomed Res Int, 2016, 2016: 4980562.
[4] Matthies C, Samii M. Management of 1000 vestibular schwannomas(acoustic neuromas): clinical presentation[J]. Neurosurgery, 1997, 40(1): 1-9.
[5] Fujiwara K, Yanagi H, Morita S, et al. Evaluation of Vertical Semicircular Canal Function in Patients With Vestibular Schwannoma[J]. Ann Otol Rhinol Laryngol, 2019, 128(2): 113-120. doi: 10.1177/0003489418808545
[6] Fife TD, Colebatch JG, Kerber KA, et al. Practice guideline: Cervical and ocular vestibular evoked myogenic potential testing: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology[J]. Neurology, 2017, 89(22): 2288-2296. doi: 10.1212/WNL.0000000000004690
[7] Papathanasiou ES, Murofushi T, Akin FW, et al. International guidelines for the clinical application of cervical vestibular evoked myogenic potentials: an expert consensus report[J]. Clin Neurophysiol, 2014, 125(4): 658-666. doi: 10.1016/j.clinph.2013.11.042
[8] Weber KP, Rosengren SM. Clinical utility of ocular vestibular-evoked myogenic potentials(oVEMPs)[J]. Curr Neurol Neurosci Rep, 2015, 15(5): 22. doi: 10.1007/s11910-015-0548-y
[9] Kiyofuji S, Neff BA, Carlson ML, et al. Large and small vestibular schwannomas: same, yet different tumors[J]. Acta Neurochir(Wien), 2021, 163(8): 2199-2207. doi: 10.1007/s00701-021-04705-6
[10] 中华耳鼻咽喉头颈外科杂志编辑委员会, 中华医学会耳鼻咽喉头颈外科学分会. 听神经瘤诊断和治疗建议[J]. 中华耳鼻咽喉头颈外科杂志, 2014, 49(3): 181-186.
[11] Xu XD, Chen BJ, Sun AR, et al. Uneven Effects of Sleep Apnea on Semicircular Canals and Otolithic Organs[J]. Front Neurol, 2022, 13: 819721. doi: 10.3389/fneur.2022.819721
[12] Nadol JB Jr, Diamond PF, Thornton AR. Correlation of hearing loss and radiologic dimensions of vestibular schwannomas(acoustic Neuromas)[J]. Am J Otol, 1996, 17(2): 312-316.
[13] Roosli C, Linthicum FH Jr, Cureoglu S, et al. Dysfunction of the cochlea contributing to hearing loss in acoustic neuromas: an underappreciated entity[J]. Otol Neurotol, 2012, 33(3): 473-480. doi: 10.1097/MAO.0b013e318248ee02
[14] Friedman RA, Kesser BW, Slattery WH 3rd, et al. Hearing preservation in patients with vestibular schwannomas with sudden sensorineural hearing loss[J]. Otolaryngol Head Neck Surg, 2001, 125(5): 544-551. doi: 10.1067/mhn.2001.119675
[15] De Donato G, Russo A, Taibah A, et al. [Incidence of normal hearing in acoustic neuroma][J]. Acta Otorhinolaryngol Ital, 1995, 15(2): 73-79.
[16] Carlson ML, Lees KA, Patel NS, et al. The Clinical Behavior of Asymptomatic Incidental Vestibular Schwannomas Is Similar to That of Symptomatic Tumors[J]. Otol Neurotol, 2016, 37(9): 1435-1441.
[17] Day AS, Wang CT, Chen CN, et al. Correlating the cochleovestibular deficits with tumor size of acoustic neuroma[J]. Acta Otolaryngol, 2008, 128(7): 756-760. doi: 10.1080/00016480701749240
[18] Patko T, Vidal PP, Vibert N, et al. Vestibular evoked myogenic potentials in patients suffering from an unilateral acoustic neuroma: a study of 170 patients[J]. Clin Neurophysiol, 2003, 114(7): 1344-1350. doi: 10.1016/S1388-2457(03)00119-6
[19] Wagner JN, Glaser M, Wowra B, et al. Vestibular function and quality of life in vestibular schwannoma: does size matter?[J]. Front Neurol, 2011, 2: 55.
[20] Kjærsgaard JB, Szeremet M, Hougaard DD. Vestibular Deficits Correlating to Dizziness Handicap Inventory Score, Hearing Loss, and Tumor Size in a Danish Cohort of Vestibular Schwannoma Patients[J]. Otol Neurotol, 2019, 40(6): 813-819.
[21] Sun W, Guo P, Ren T, et al. Magnetic resonance imaging of intratympanic gadolinium helps differentiate vestibular migraine from Ménière disease[J]. Laryngoscope, 2017, 127(10): 2382-2388.
[22] Guo P, Sun W, Shi S, et al. Quantitative evaluation of endolymphatic hydrops with MRI through intravenous gadolinium administration and VEMP in unilateral definite Meniere's disease[J]. Eur Arch Otorhinolaryngol, 2019, 276(4): 993-1000.
[23] Lin KL, Chen CM, Wang SJ, et al. Correlating vestibular schwannoma size with vestibular-evoked myogenic potential results[J]. Ear Hear, 2014, 35(5): 571-576.
[24] Zhou Y, Zhao W, Tian L, et al. The prediction of the tumor size of a vestibular schwannoma by clinical performance and vestibular function tests[J]. J Neurooncol, 2018, 140(3): 679-686.
[25] Fröhlich L, Curthoys IS, Kösling S, et al. Cervical and Ocular Vestibular-Evoked Myogenic Potentials in Patients With Intracochlear Schwannomas[J]. Front Neurol, 2020, 11: 549817.
[26] Brown CS, Peskoe SB, Risoli T Jr, et al. Associations of Video Head Impulse Test and Caloric Testing among Patients with Vestibular Schwannoma[J]. Otolaryngol Head Neck Surg, 2019, 161(2): 324-329.
[27] 徐先荣, 金占国, 翟丽红, 等. 前庭感受器病——一种尚未认知的外周前庭疾病及航空医学鉴定[J]. 空军医学杂志, 2022, 38(1): 1-4.
[28] Nilsen KS, Nordahl S, Berge JE, et al. Vestibular Tests Related to Tumor Volume in 137 Patients With Small to Medium-Sized Vestibular Schwannoma[J]. Otolaryngol Head Neck Surg, 2023, 169(5): 1268-1275.
[29] Fujiwara K, Morita S, Fukuda A, et al. Analysis of semicircular canal function as evaluated by video Head Impulse Test in patients with vestibular schwannoma[J]. J Vestib Res, 2020, 30(2): 101-108.
[30] Blödow A, Helbig R, Wichmann N, et al. [Video head impulse test or caloric irrigation? Contemporary diagnostic tests for vestibular schwannoma][J]. HNO, 2013, 61(9): 781-785.
[31] 邹曙光, 毛秋月, 彭安全, 等. 视频头脉冲试验、冷热试验和眩晕障碍程度评定量表诊断听神经瘤的价值[J]. 临床耳鼻咽喉头颈外科杂志, 2022, 36(8): 613-616. https://lceh.whuhzzs.com/article/doi/10.13201/j.issn.2096-7993.2022.08.009
-
图(3)
表(5)
计量
- 文章访问数: 403
- PDF下载数: 52
- 施引文献: 0