
Effect and differentiation of spontaneous nystagmus of acute unilateral vestibulopathy on saccade in the video head impulse test
-
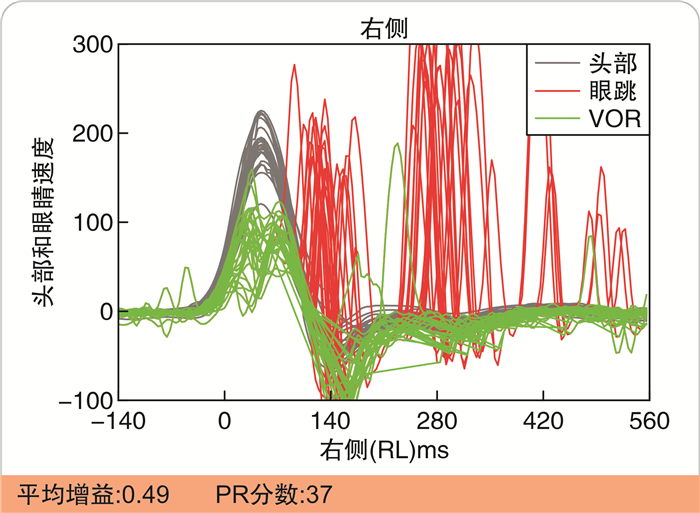
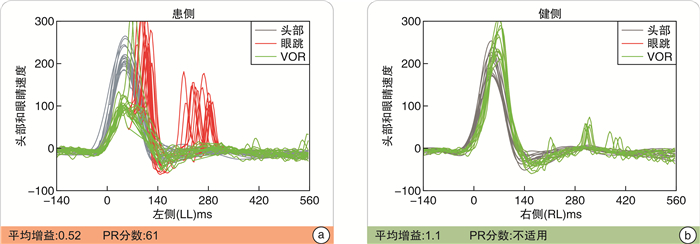
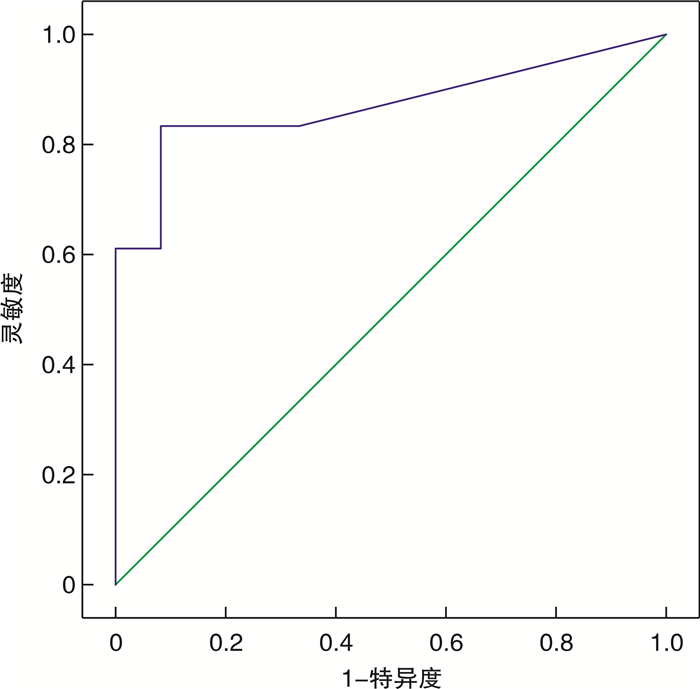
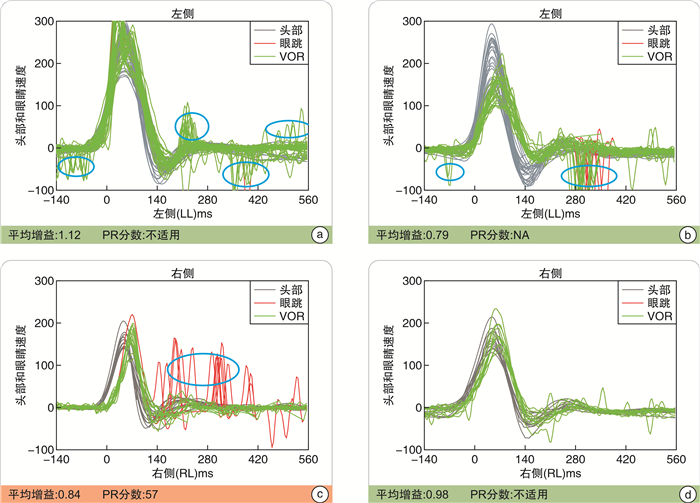
摘要: 目的 探究急性单侧前庭病自发性眼震(spontaneous nystagmus,SN)在视频头脉冲试验(video-head impulse test,vHIT)中的表现特征及其对扫视眼动的影响。方法 对48例急性单侧前庭病(acute unilateral vestibulopathy,AUVP)患者进行vHIT及SN等前庭功能检查,分别分析无SN与存在SN患者的vHIT扫视波特征以及SN在vHIT中的表现特征。结果 48例AUVP患者中,存在SN者34例,其中健侧出现扫视31例,与眼动方向同向和反向均有的11例,仅有反向19例,仅同向1例,3例无扫视。无SN患者14例,其中健侧出现扫视10例,其中与眼动同向和反向均有的4例,仅有反向2例,仅有同向4例,无扫视4例。健侧是否出现反向扫视与患者是否存在SN具有相关性。SN在vHIT中可在健侧表现为与眼动方向相反,而在患侧可表现为与眼动方向相同并且可能使显性扫视更加离散。急性期(病程≤2 w)32例,存在SN的患者29例,SN强度为(6.7±3.2)°/s,3例无SN。恢复期(病程>2 w)16例,存在SN的患者5例,SN强度为(3.7±2.1)°/s,11例无SN。在急性期中健侧出现扫视30例,与眼动方向同向和反向均有10例,仅有反向18例,仅有同向2例,无扫视2例。病程时期与健侧是否会出现反向扫视具有相关性。健侧水平半规管vHIT出现反向扫视的SN强度cut off点为2.1°/s。结论 AUVP患者的vHIT多存在波形相似的补偿扫视和SN,SN波在健侧与眼动波方向相反、患侧与显性扫视方向同向混合在一起,可对vHIT显性扫视的离散度及振幅构成影响。准确辨别AUVP患者vHIT中的SN,不但是识别补偿扫视的关键,也可对AUVP诊断及代偿评估提供帮助。Abstract: Objective Exploring the performance characteristics of spontaneous nystagmus(SN) in video-head impulse test(vHIT) and its possible effects on saccade.Methods Vestibular function tests such as vHIT and SN were conducted in 48 patients with acute unilateral vestibulopathy(AUVP). The saccade characteristics of vHIT in patients without SN and those with SN were analyzed, as well as the expression characteristics of SN in vHIT.Results Among the 48 AUVP patients, there were 34 cases with SN, including 31 cases with saccade on the healthy side, 11 cases with both the same and opposite directions of eye movement, 19 with the opposite only, 1 with same direction only, and 3 cases without saccade. There were 14 patients without SN, of whom 10 showed saccade on the healthy side, including 4 with both eye movements in the same and opposite direction, 2 in the opposite direction only, 4 in the same direction only, and 4 without saccade. There is a correlation between reverse saccade on the healthy side and the presence of SN in patients. SN in vHIT can appear opposite to the direction of eye movement on the healthy side, while on the affected side it can appear the same as the direction of eye movement and may cause more discrete overt saccade. 32 patients in the acute phase(≤2 w), 29 patients with SN, SN intensity of(6.7 ± 3.2) °/s, and 3 patients without SN. 16 cases in non acute phase(>2 w), 5 cases with SN, SN intensity of(3.7 ± 2.1) °/s, and 11 cases without SN. In the acute phase there were 30 cases of saccade on the healthy side, 10 cases with both the same and opposite direction of eye movement, 18 cases with only the opposite direction, 2 cases with only the same direction and 2 cases without saccade. There is a correlation between the duration of the disease and the occurrence of reverse saccade on the healthy side. The intensity cut off point of SN for reverse saccade is 2.1 °/s in the healthy lateral semicircular canal vHIT.Conclusion Compensatory saccades and SN waves with similar waveforms are mostly present in vHIT in AUVP patients. SN wave is in the opposite direction of the normal side and eye movement wave, and the affected side and dominant saccade direction are in the same direction and mixed together, which can affect the dispersion and amplitude of overt saccade in vHIT. Accurate identification of SN in vHIT of AUVP patients is not only the key factor to identify compensatory saccade, but also can provide help for the diagnosis and compensatory assessment of AUVP.
-

-
表 1 病程与健侧水平半规管反向扫视的相关性
病程 例数 健侧出现反向扫视 其他+无扫视
(无反向扫视)急性期 32 28 4 恢复期 16 8 8 t=6.125 P=0.013  下载: 导出CSV
下载: 导出CSV
-
[1] Strupp M, Brandt T. Vestibular neuritis[J]. Semin Neurol, 2009, 29(5): 509-519. doi: 10.1055/s-0029-1241040
[2] Strupp M, Brandt T. Peripheral vestibular disorders[J]. Curr Opin Neurol, 2013, 26(1): 81-89. doi: 10.1097/WCO.0b013e32835c5fd4
[3] Alhabib SF, Saliba I. Video head impulse test: a review of the literature[J]. Eur Arch Otorhinolaryngol, 2017, 274(3): 1215-1222. doi: 10.1007/s00405-016-4157-4
[4] Du Y, Ren L, Liu X, et al. The characteristics of vHIT gain and PR score in peripheral vestibular disorders[J]. Acta Otolaryngol, 2021, 141(1): 43-49. doi: 10.1080/00016489.2020.1812715
[5] Strupp M, Bisdorff A, Furman J, et al. Acute unilateral vestibulopathy/vestibular neuritis: Diagnostic criteria[J]. J Vestib Res, 2022, 32(5): 389-406. doi: 10.3233/VES-220201
[6] 中国医师协会神经内科分会眩晕专业委员会, 中国卒中学会卒中与眩晕分会. 前庭神经炎诊治多学科专家共识[J]. 中华老年医学杂志, 2020, 39(9): 985-994. doi: 10.3760/cma.j.issn.0254-9026.2020.09.001
[7] Blödow A, Pannasch S, Walther LE. Detection of isolated covert saccades with the video head impulse test in peripheral vestibular disorders[J]. Auris Nasus Larynx, 2013, 40(4): 348-351. doi: 10.1016/j.anl.2012.11.002
[8] Cremer PD, Halmagyi GM, Aw ST, et al. Semicircular canal plane head impulses detect absent function of individual semicircular canals[J]. Brain, 1998, 121(Pt 4): 699-716.
[9] Psillas G, Petrou I, Printza A, et al. Video Head Impulse Test(vHIT): Value of Gain and Refixation Saccades in Unilateral Vestibular Neuritis[J]. J Clin Med, 2022, 11(12): 3467. doi: 10.3390/jcm11123467
[10] Fu W, He F, Wei D, et al. Recovery Pattern of High-Frequency Acceleration Vestibulo-Ocular Reflex in Unilateral Vestibular Neuritis: A Preliminary Study[J]. Front Neurol, 2019, 10: 85. doi: 10.3389/fneur.2019.00085
[11] Manzari L, Graziano D, Tramontano M. The Different Stages of Vestibular Neuritis from the Point of View of the Video Head Impulse Test[J]. Audiol Res, 2020, 10(2): 31-38. doi: 10.4081/audiores.2020.248
[12] Riska KM, Bellucci J, Garrison D, et al. Relationship Between Corrective Saccades and Measures of Physical Function in Unilateral and Bilateral Vestibular Loss[J]. Ear Hear, 2020, 41(6): 1568-1574. doi: 10.1097/AUD.0000000000000885
-
图(4)
表(2)
计量
- 文章访问数: 369
- PDF下载数: 18
- 施引文献: 0