
Classification and surgical strategy of Work Ⅰ congenital first branchial cleft anomaly based on adjacent anatomy
-
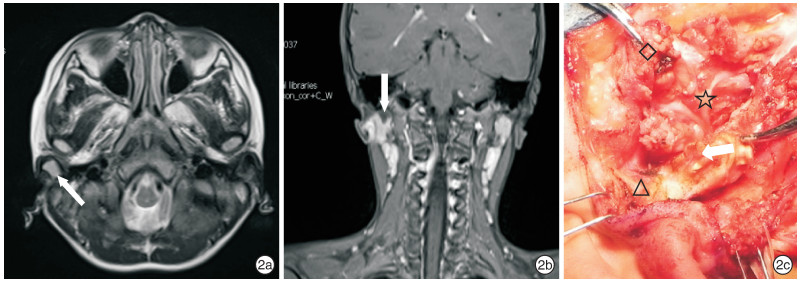
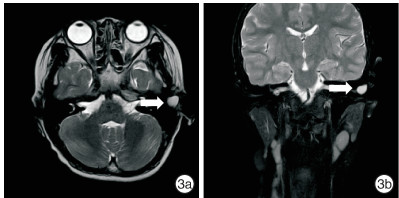
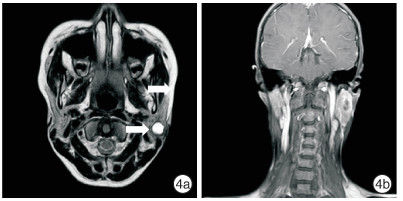
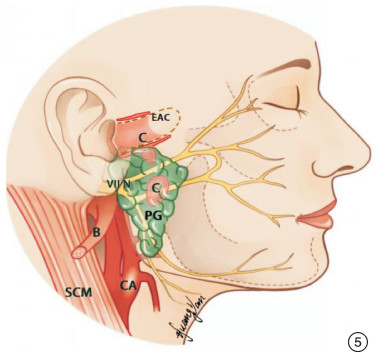
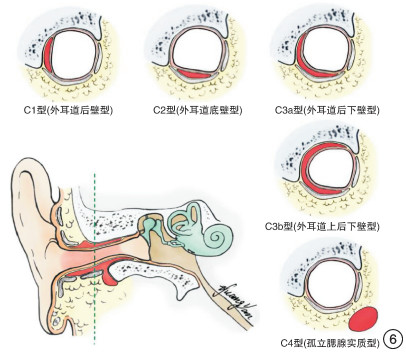
摘要: 目的 探讨Work Ⅰ型先天性第一鳃裂畸形(CFBCA)的区域毗邻解剖关系及分型。 方法 回顾性分析资料完整的48例Work Ⅰ型CFBCA资料。 结果 48侧病损均完整切除;48侧(100%)均解剖保留面神经;33侧(68.8%)行腮腺部分切除、9侧(18.8%)行腮腺浅叶+深叶部分切除、6侧(12.5%)未行腮腺切除;32侧(66.7%)行外耳道重建;43侧(89.6%)行耳大神经耳垂支解剖保留;9侧(18.8%)同期行择区颈清。45侧Work Ⅰ型CFBCA呈不规则囊状或分叶结构,病损主体位于外耳道骨与软骨交汇处后下方,沿外耳道纵轴分布;3侧孤立于腮腺浅叶实质内。所有病损均位于面神经主干及分支浅面,病损下缘与面神经主干出茎乳孔处的最短垂直距离平均值7.2(0~13.4)mm。基于术前影像及术中所见,根据病损与外耳道、腮腺和面神经的毗邻关系,提出Work Ⅰ型先天性第一鳃裂畸形的分型,具体分为4型:C1型(外耳道后壁型)17例(35.4%)、C2型(外耳道底壁型)13例(27.1%)、C3型(外耳道多壁型)15例(31.3%)、C4型(孤立于腮腺实质型)3例(6.3%)。 结论 Work Ⅰ型CFBCA与区域毗邻解剖关系密切,熟悉Work Ⅰ型先天性第一鳃裂畸形的分型,有助于因型施治、精准切除。Abstract: Objective To explore the adjacent anatomic relationship and classification of Work Ⅰ congenital first branchial cleft anomaly(CFBCA) in order to guide clinical practice. Method The data of 48 cases of Work Ⅰ CFBCA with complete data were analyzed retrospectively. Result All 48 lesions were completely resected. 48 sides(100.0%) were anatomically preserved facial nerve, partial parotidectomy was performed on 33 sides(68.8%), superficial lobe+deep lobe partial parotidectomy was performed on 9 sides(18.8%), and 6 sides(12.5%) was not performed parotidectomy. External auditory canal reconstruction was performed on 32 sides(66.7%); 43 sides(89.6%) underwent the anatomical preservation of the auricular lobe branch of the great auricular nerve; 9 sides(18.8%) was performed selective cervical lymphadenectomy at the same time. 45 sides of Work Ⅰ CFBCA presented irregular cystic or lobulated structure, the lesion was located below and behind the junction of the external auditory meatus bone and cartilage and distributed along the longitudinal axis of the external auditory canal; 3 sides were isolated in superficial lobe parenchyma of parotid gland. All lesions were located on the superficial surface of the main trunk and branches of the facial nerve. The average value of the shortest vertical distance between the lower edge of the lesion and the outlet of the main trunk of the facial nerve at the stylomastoid foramen was 7.2 (0-13.4)mm. Based on preoperative images and intraoperative findings, according to the adjacent relation with external auditory meatus, parotid gland and facial nerve, the classification of Work Ⅰ congenital first branchial cleft anomaly is proposed, which is specifically divided into 4 types: C1(posterior wall of the external auditory meatus) 17 cases(35.4%), C2(inferior wall of the external auditory meatus) 13 cases(27.1%), C3 (multi wall of the external auditory meatus) 15 cases(31.3%), C4(isolated from parotid gland parenchyma) 3 cases(6.3%). Conclusion Work Ⅰ CFBCA has a close relationship with the adjacent anatomy of the region, and familiar with the classification of Work Ⅰ congenital first branchial cleft anomaly is helpful for the treatment of type and accurate resection.
-

-
表 1 Work Ⅰ型CFBCA的分型与区域毗邻解剖的关系
分型 例数(%) 与外耳道关系 与腮腺关系 与面神经关系 病损下缘与面神经主干出茎乳孔最短距离平均值/mm 与耳大神经耳垂支关系 C1型(后壁型) 17(35.4) 仅与外耳道后壁共壁 毗邻腮腺后缘 浅面 10.6 深面 C2型(底壁型) 13(27.1) 仅与外耳道底壁共壁 毗邻或侵入腮腺实质 浅面 7.7 深面 C3型(多壁型) C3a(毗邻后壁和底壁) 15(31.3) 与外耳道多壁相邻,呈90~270°包绕 侵入腮腺实质 浅面 2.3 深面 C3b(毗邻后壁、上壁及底壁) C4型(孤立型) 3(6.2) 与外耳道四壁均无关联 孤立位于腮腺实质内 浅面 10.6 深面  下载: 导出CSV
下载: 导出CSV
-
[1] Arndal H, Bonding P.First branchial cleft anomaly[J]. Clin Otolaryngol Allied Sci, 1996, 21(3):203-207. doi: 10.1111/j.1365-2273.1996.tb01725.x
[2] Work WP.Newer concepts of first branchial cleft defects[J]. Laryngoscope, 1972,125(3):520-532.
[3] Olivas AD, Sherman JM.First branchial cleft anomalies[J]. Oper Tech Otolayngol Head Neck Surg, 2017, 28(3):151-155. doi: 10.1016/j.otot.2017.05.012
[4] Liu W, Chen M, Hao J, et al.The treatment for the first branchial cleft anomalies in children[J]. Eur Arch Otorhinolaryngol, 2017,274(9):3465-3470. doi: 10.1007/s00405-017-4648-y
[5] Triglia JM, Nicollas R, Ducroz V, et al.First branchial cleft anomalies:a study of 39 cases and a review of the literature[J]. Arch Otolaryngol Head Neck Surg, 1998,124(3):291-295. doi: 10.1001/archotol.124.3.291
[6] Kumar R, Sikka K, Sagar P, et al.First branchial cleft anomalies:avoiding the misdiagnosis[J]. Indian J Otolaryngol Head Neck Surg, 2013, 65(3):260-263. doi: 10.1007/s12070-013-0641-y
[7] Del Pero MM, Majumdar S, Bateman N, et al.Presentation of first branchial cleft anomalies:the Sheffield experience[J]. J Laryngol Otol, 2007,121(5):455-459. doi: 10.1017/S0022215106004373
[8] D'Souza AR, Uppal HS, De R, et al.Updating concepts of first branchial cleft defects:a literature review[J]. Int J Pediatr Otorhinolaryngol, 2002, 62(2), 103-109. doi: 10.1016/S0165-5876(01)00612-7
[9] 钟贞, 赵恩民, 刘玉和, 等.先天性第一鳃裂畸形的诊治和分类[J].临床耳鼻咽喉头颈外科杂志, 2013, 27(13):691-694. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH201313007.htm
[10] Ertas B, Gunaydin RO, Unal OF.The relationship between the fistula tract and the facial nerve in type Ⅱ first branchial cleft anomalies[J]. Auris Nasus Larynx, 2015, 42(2):119-122. doi: 10.1016/j.anl.2014.08.017
[11] Chan KC, Chao WC, Wu CM.Surgical management of first branchial cleft anomaly presenting as infected retroauricular mass using a microscopic dissection technique[J]. Am J Otolaryngol, 2012, 33(1):20-25. doi: 10.1016/j.amjoto.2010.12.003
[12] Schroeder JW Jr, Mohyuddin N, Maddalozzo J.Branchial Anomalies in the Pediatric Population[J]. Otolaryngol Head Neck Surg, 2016,137(2):289-295.
[13] 李波, 邹剑, 郑虹, 等.第一鳃裂瘘管切除术中面神经解剖的临床意义[J].中国耳鼻咽喉头颈外科, 2012, 19(4):179-181. https://www.cnki.com.cn/Article/CJFDTOTAL-EBYT201204006.htm
[14] Olsen K D, Maragos N E, Weiland L H. First branchial cleft anomalies[J]. Laryngoscope, 1980, 90(3):423-436. doi: 10.1002/lary.5540900309
[15] 张贝, 陈良嗣, 黄舒玲, 等.Work Ⅱ型先天性第一鳃裂畸形与面神经解剖关系研究及外科策略[J].中华耳鼻咽喉头颈外科杂志, 2017, 52(10):760-765. doi: 10.3760/cma.j.issn.1673-0860.2017.10.009
[16] Aronsohn RS, Batsakis JG, Rice DH, et al.Anomalies of the first branchial cleft[J]. Arch Otolaryngol, 1976,102(12):737-740. doi: 10.1001/archotol.1976.00780170055008
[17] Maithani T, Pandey A, Dey D, et al.First branchial cleft anomaly:clinical insight into its relevance in otolaryngology with pediatric considerations[J]. Indian J Otolaryngol Head Neck Surg, 2014, 66(S1):271-276. doi: 10.1007/s12070-012-0482-0
[18] Arnot RS.Defects of the first branchial cleft[J]. S Afr J Surg, 1971, 9(2):93-98.
[19] 俞光岩, 马大权.功能性腮腺外科[J].中国肿瘤临床, 2010, 37(16):908-910. doi: 10.3969/j.issn.1000-8179.2010.16.003
[20] 陈敏, 郑美君, 李文, 等.儿童第一鳃裂畸形术中耳大神经的保护[J].华西医学, 2018, 33(3):321-324. https://www.cnki.com.cn/Article/CJFDTOTAL-HXYX201803018.htm
[21] Guntinas-Lichius O, Silver CE, Thielker J, et al.Management of the facial nerve in parotid cancer:preservation or resection and reconstruction[J]. Eur Arch Otorhinolaryngol, 2018,275(11):2615-2626. doi: 10.1007/s00405-018-5154-6
[22] 张贝, 陈良嗣, 黄舒玲, 等.先天性第一鳃裂畸形临床特点分析:附56例报告[J].临床耳鼻咽喉头颈外科杂志, 2016(17):1359-1362.. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH201617005.htm
[23] 陈良嗣, 宋新汉, 张思毅, 等.择区性颈清扫术治疗复发性鳃裂畸形[J].临床耳鼻咽喉头颈外科杂志, 2011, 25(2):51-53. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH201102004.htm
-
图(6)
表(1)
计量
- 文章访问数: 1450
- PDF下载数: 564
- 施引文献: 0