
-
摘要: 目的 探索内听道少见肿瘤手术过程中面神经保护的策略。方法 纳入2010至2023年就诊的235例内听道肿瘤患者, 其中包括前庭神经鞘瘤、海绵状血管瘤、脑膜瘤等少见肿瘤。通过临床表现、影像学分类和治疗过程等多方面数据, 详细分析少见肿瘤的特点, 术前术后的面神经功能情况。结果 在所有内听道肿瘤中, 前庭神经鞘瘤占91.9%;在少见肿瘤中, 面神经鞘瘤占5.3%, 海绵状血管瘤占26.3%, 脑膜瘤占15.8%, 动脉瘤占10.5%。海绵状血管瘤患者中肿瘤侵袭面神经的情况明显, 而其他肿瘤与面神经边界清晰。手术过程中, 对于不同类型的肿瘤, 采取了个体化的手术入路和面神经保护策略, 包括术中分离、肿瘤切除、面神经重建等。结论 面神经在内听道少见肿瘤手术中的保护至关重要。通过精准的术前诊断、合适的手术时机、选择性的手术入路以及术中的细致操作, 可以最大限度地保护面神经功能。个体化的治疗方案和面神经功能的重建策略有望提高手术成功率, 减轻患者术后面神经功能障碍的风险, 从而改善患者的生活质量。Abstract: Objective To explore strategies for preserving facial nerve function during surgeries for rare tumors of the internal auditory canal.Methods A total of 235 cases of internal auditory canal tumors treated between 2010 and 2023 were included, encompassing vestibular schwannomas, cavernous hemangiomas, meningiomas, and other rare tumors. Various data, including clinical presentations, imaging classifications, and treatment processes, were meticulously analyzed to delineate the characteristics of rare tumors and assess pre-and postoperative facial nerve function.Results Among all internal auditory canal tumors, vestibular schwannomas accounted for 91.9%. In rare tumors, facial nerve schwannomas constituted 5.3%, cavernous hemangiomas 26.3%, meningiomas 15.8%, and arterial aneurysms 10.5%. Significantly, patients with cavernous hemangiomas displayed pronounced invasion of the facial nerve by the tumor, in contrast to other tumor types where clear boundaries with the facial nerve were maintained. During surgery, individualized approaches and strategies for facial nerve protection were implemented for different tumor types, involving intraoperative dissection, tumor excision, and facial nerve reconstruction.Conclusion Preservation of the facial nerve is crucial in the surgical management of rare tumors of the internal auditory canal. Accurate preoperative diagnosis, appropriate timing of surgery, selective surgical approaches, and meticulous intraoperative techniques can maximize the protection of facial nerve function. Personalized treatment plans and strategies for facial nerve functional reconstruction are anticipated to enhance surgical success rates, reduce the risk of postoperative facial nerve dysfunction, and ultimately improve the quality of life for patients.
-

-
表 1 不同类型IAC肿瘤的人数及首发症状及发生率
肿瘤类型 总例数 听力下降 眩晕 面神经功能障碍 例数 发生率/% 例数 发生率/% 例数 发生率/% VS 216 213 98.6 32 14.8 21 9.7 少见肿瘤 19 18 94.7 4 21.1 11 57.9 AICAA 2 2 100.0 1 50.0 2 100.0 IAC-M 3 3 100.0 1 100.0 1 33.3 ILS 1 1 100.0 1 100.0 0 0 IAC-CH 5 5 100.0 0 0 4 80.0 FNS 1 1 100.0 1 100.0 1 100.0 NF2 5 4 80.0 0 0 2 40.0 胆脂瘤 2 2 100.0 0 0 1 50.0 合计 235 231 98.2 36 15.3 32 13.6  下载: 导出CSV
下载: 导出CSV
表 2 IAC肿瘤典型病例资料
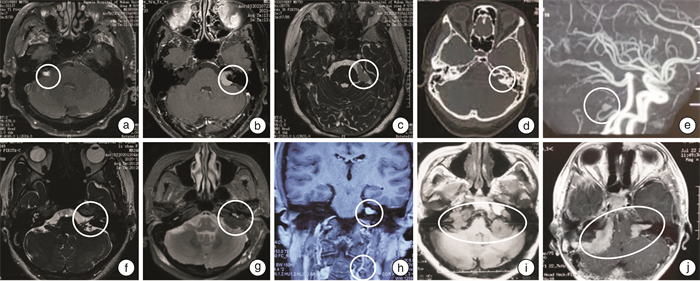
序号 性别 年龄/岁 临床表现 发病时间 影像学表现 诊断 治疗措施 随访时间 预后 1 男 46 右侧重度听力下降,面神经功能障碍(HB分级4级) 10年 MRI:右侧内听道肿瘤,肿瘤内不均匀强化(图 2a) IAC-CH 经迷路入路病变切除 2年 患侧无实用听力,面神经功能HB分级4级 2 女 65 左侧重度听力下降,眩晕,面神经功能障碍(HB分级1级) 3个月 MRI:左侧内听道肿瘤,可见脑膜尾症(图 2b) IAC-M 经迷路入路病变切除 1.5年 患侧无实用听力,眩晕症状消失,面神经功能正常 3 女 67 耳鸣,三叉神经痛,面神经功能障碍(HB分级3级) 1个月 MRI:左侧内听道及桥小脑角肿瘤,未见增强(图 2c) 胆脂瘤 窦后入路病变切除术 1年 患侧轻度听力下降,面神经功能HB分级2级 4 女 62 左侧极重度听力下降,眩晕,面肌痉挛 3个月 CT:左侧内听道占位,壶腹样扩张(图 2d);MRA:左侧小脑前下动脉动脉瘤(图 2e) AICAA 经迷路入路动脉瘤夹闭+病变切除 5年 患侧无实用听力,眩晕症状明显减轻,面神经功能HB分级1级 5 女 34 左侧极重度听力下降、耳鸣,眩晕 10年 MRI:左侧耳蜗、前庭、内听道肿瘤(图 2f) ILS 经迷路入路病变切除 1年 患侧无实用听力,眩晕症状消失 6 女 38 左侧极重度听力下降,眩晕,面神经麻痹(HB分级3级) 2个月 MRI:左侧内听道肿瘤(图 2g) FNS 经迷路入路病变切除+面神经吻合术 1年 患侧无实用听力,眩晕症状小时,面神经功能HB分级3级 7 男 22 左侧轻度听力下降、耳鸣 2个月 MRI:左侧内听道肿瘤,颈部神经源性肿瘤(图 2h) NF2 随访观察 3年 听力水平、肿瘤未见明显变化 8 男 29 双侧听力下降,双侧面神经功能障碍(HB分级3级) 10年 MRI:双侧内听道及桥小脑角肿瘤(图 2i) NF2 右侧带瘤人工耳蜗植入术 4年 人工耳蜗开机后可听到敲击桌子的声音,面神经功能如前 9 男 16 双侧听力下降,双侧面神经功能障碍(HB分级3级) 3年 MRI:双侧内听道及桥小脑角肿瘤,脑干受压(图 2j) NF2 双侧内听道及桥小脑角病变切除术+人工听觉脑干植入术 15年 可在安静情况下结合唇语交流,面神经功能如前 10 女 57 左侧极重度听力下降、耳鸣、面神经功能障碍(HB分级2级) 6个月 MRI:内听道肿瘤 VS 经迷路入路病变切除术+面神经吻合术 1年 患侧无实用听力,面神经功能HB分级3级
下载: 导出CSV
表 3 IAC少见肿瘤的临床特点和影像学特点
肿瘤类型 临床特点 影像学特点 IAC-CH 大部分患者早期即出现面神经功能障碍[7] CT:骨质侵犯、瘤内点状钙等[7] IAC-M 11.4%的患者术前即出现面神经功能障碍[8] MRI:脑膜尾征 AICAA 多以蛛网膜下腔出血为首发症状[9] CT:内听道“壶腹样”扩大;血管成像可确诊[2] ILS 早期即出现难治性眩晕 MRI:病变侵犯迷路[10] 胆脂瘤 三叉神经痛[11] CT:骨质不规则破坏,MRI:T1低信号,T2高信号,肿瘤不强化[12] FNS 很难术前鉴别,需要术中探查确诊 NF2 青少年发病,双侧内听道肿瘤[13] MRI:多种肿瘤类型混合的肿瘤(神经纤维瘤、神经鞘瘤、脑膜瘤、室管膜瘤等)
下载: 导出CSV
-
[1] Benson JC, Carlson ML, Lane JI. MRI of the Internal Auditory Canal, Labyrinth, and Middle Ear: How We Do It[J]. Radiology, 2020, 297(2): 252-265. doi: 10.1148/radiol.2020201767
[2] 杨冰倩, 杨希林, 吴展元, 等. 内听道少见肿瘤[J]. 中华耳鼻咽喉头颈外科杂志, 2022, 57(7): 843-847.
[3] Sykopetrites V, Piras G, Taibah A, et al. Meningiomas of the Internal Auditory Canal[J]. Laryngoscope, 2021, 131(2): E413-E419.
[4] 吴南, 王方园, 侯昭晖, 等. 局限于内听道及桥小脑角的面神经肿瘤临床分析[J]. 中华耳科学杂志, 2019, 17(3): 330-333. https://www.cnki.com.cn/Article/CJFDTOTAL-ZHER201903010.htm
[5] Watanabe K, Cobb M, Zomorodi AR, et al. Rare Lesions of the Internal Auditory Canal[J]. World Neurosurg, 2017, 99: 200-209. doi: 10.1016/j.wneu.2016.12.003
[6] Dazert S, Aletsee C, Brors D, et al. Rare tumors of the internal auditory canal[J]. Eur Arch Otorhinolaryngol, 2005, 262(7): 550-554. doi: 10.1007/s00405-003-0734-4
[7] Zhu WD, Huang Q, Li XY, et al. Diagnosis and treatment of cavernous hemangioma of the internal auditory canal[J]. J Neurosurg, 2016, 124(3): 639-646. doi: 10.3171/2015.3.JNS142785
[8] Sykopetrites V, Taibah A, Piras G, et al. The otologic approach in the management of posterior petrous surface meningiomas[J]. Eur Arch Otorhinolaryngol, 2022, 279(12): 5655-5665. doi: 10.1007/s00405-022-07442-3
[9] 范罡贤, 刘鹏飞, 高文波, 等. 内镜下夹闭内听道内动脉瘤二例报道[J]. 中华神经医学杂志, 2021, 20(1): 85-85.
[10] 王恩彤, 单希征. 迷路内神经鞘瘤的研究进展[J]. 中华耳鼻咽喉头颈外科杂志, 2020, 55(7): 707-707.
[11] 张永强, 于峰, 门学忠, 等. 桥小脑角区胆脂瘤继发三叉神经痛[J]. 中国微侵袭神经外科杂志, 2021, 26(4): 175-176. https://www.cnki.com.cn/Article/CJFDTOTAL-ZWQX202104014.htm
[12] Migirov L, Bendet E, Kronenberg J. Cholesteatoma invasion into the internal auditory canal[J]. Eur Arch Otorhinolaryngol, 2009, 266(5): 657-662. doi: 10.1007/s00405-008-0804-8
[13] Dinh CT, Nisenbaum E, Chyou D, et al. Genomics, Epigenetics, and Hearing Loss in Neurofibromatosis Type 2[J]. Otol Neurotol, 2020, 41(5): e529-e537. doi: 10.1097/MAO.0000000000002613
[14] 徐茂翔, 姜雨萌, 姚青秀, 等. 听神经瘤的非手术治疗研究进展[J]. 临床耳鼻咽喉头颈外科杂志, 2022, 36(12): 971-976. https://lceh.whuhzzs.com/article/doi/10.13201/j.issn.2096-7993.2022.12.017
[15] 李智慧, 吕佳蕙, 陈纲, 等. 突发性感音神经性听力损失与内听道MRI中面听神经及小脑前下动脉血管袢的相关性研究[J]. 临床耳鼻咽喉头颈外科杂志, 2022, 36(6): 435-440. https://lceh.whuhzzs.com/article/doi/10.13201/j.issn.2096-7993.2022.06.006
[16] Schwam ZG, Cosetti MK, Wanna GB. Translabyrinthine Approach for Sporadic Vestibular Schwannoma: Patient Selection, Technical Pearls, and Patient Outcomes[J]. Otolaryngol Clin North Am, 2023, 56(3): 483-493. doi: 10.1016/j.otc.2023.02.008
[17] Lucas JC, Fan CJ, Jacob JT, et al. Retrosigmoid Approach for Sporadic Vestibular Schwannoma: Patient Selection, Technical Pearls, and Hearing Results[J]. Otolaryngol Clin North Am, 2023, 56(3): 509-520. doi: 10.1016/j.otc.2023.02.010
[18] Peris-Celda M, Perry A, Carlstrom LP, et al. Key anatomical landmarks for middle fossa surgery: a surgical anatomy study[J]. J Neurosurg, 2018: 1-10.
[19] Bien AG, Kim CS, Kenning TJ. Temporal Bone and Cerebellopontine Angle Epidermoid Resulting in Facial Nerve Paralysis: Resection and Facial Nerve Coaptation[J]. J Neurol Surg B Skull Base, 2019, 80(Suppl 3): S314-S315.
-
计量
- 文章访问数: 183
- 施引文献: 0