
Effects of mouth opening breathing for different reasons on maxillofacial development in children
-
摘要: 目的 探究不同原因张口呼吸对儿童颌面部发育的影响。方法 选择151例患儿作为研究对象。依据不同病因将其分为49例腺样体肥大组(A组)、52例扁桃体肥大组(B组)、50例腺样体伴扁桃体肥大组(C组)。选择同期的健康儿童作为本次试验的对照组,共45例。分析A组、B组、C组与对照组的反射鼻咽腔测量参数、面部发育指标及头影参数,研究A组、B组、C组安氏Ⅱ类、安氏Ⅲ类的发生率。结果 A组、B组、C组的反射鼻咽腔测量参数与对照组比较,差异有统计学意义(P < 0.05),头影参数发生改变且各组间不同(P < 0.05)。A组和C组的安氏Ⅱ类发生率较高,B组和C组的安氏Ⅲ类发生率较高(P < 0.05)。结论 腺样体肥大会导致下颌骨后缩,扁桃体肥大会造成下颌前伸,腺样体肥大及扁桃体肥大均容易导致下颌骨出现顺时针旋转的状态。为避免患儿发育不协调,临床应尽早对患儿的颌面部情况进行纠正。Abstract: Objective To explore the effects of mouth opening breathing for different reasons on children's maxillofacial development.Methods One hundred and fifty-one children were selected as the research objects of this experiment. They were divided into 49 cases of adenoid hypertrophy group(group A), 52 cases of tonsillar hypertrophy group(group B) and 50 cases of adenoid with tonsillar hypertrophy group(Group C). Healthy children in the same period were selected as the control group, a total of 45 cases. The reflex nasopharyngeal measurement parameters, facial development indexes and cephalometric parameters of group A, group B, group C and control group were analyzed, and the incidence of Angle ClassⅡand Angle Class Ⅲ in group A, group B and group C were studied.Results Compared with the control group, the reflex nasopharyngeal measurement parameters in group A, group B and group C was significantly different(P < 0.05), and the cephalometric parameters changed with variation in groups(P < 0.05). The incidence of Angle Class Ⅱ facial pattern in group A and group C was higher, but the incidence of Angle Class Ⅲ facial pattern in group B and group C was higher(P < 0.05).Conclusion Adenoid hypertrophy leads to mandibular retraction; tonsil hypertrophy leads to anterior mandibular arch; adenoid hypertrophy and tonsil hypertrophy are easy to lead to clockwise rotation of the mandible. In clinical practice, to avoid children's uncoordinated maxillofacial development, we should correct the maxillofacial situation of children as soon as possible.
-

-
表 1 头影参数指标意义
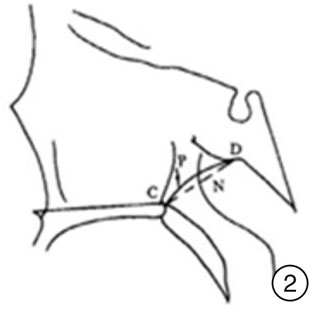
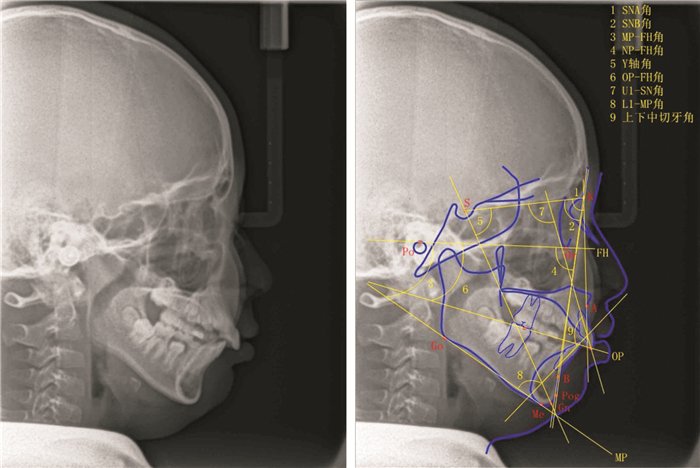
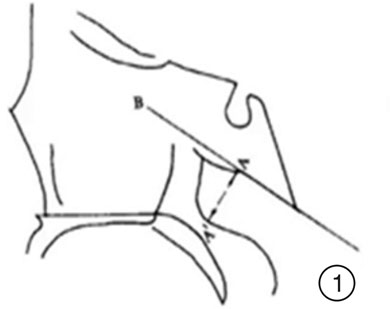
头影参数 定义 临床意义 SNA角 由蝶鞍中心、鼻根点及上牙槽座点所构成的角 反映上颌相对于颅部的前后位置关系;当此角过大时,上颌前突、面部侧貌可呈凸面型,反之上颌后缩面部呈凹面型 SNB角 由蝶鞍中心、鼻根点及下牙槽座点所构成的角 反映下颌相对于颅部的前后位置关系;此角过大时,下颌呈前突,反之下颌呈后缩 MP-FH角 由下颌平面(MP)与眼耳平面(FH)的交角 代表下颌体的陡度,下颌角的大小,也反映面部的高度 NP-FH角 面平面(NP)与眼耳平面(FH)相交的后下角 反映下颌的突缩程度;此角越大表示下颌越前突,反之则表示下颌后缩 Y轴角 蝶鞍中心与颏顶点连线(SGn)与眼耳平面(FH)相交的下前角 此角反映颏部的突缩;此角越小则表示颏部越突,反之则表示颏部越缩 OP-FH角 合平面(OP)与眼耳平面(FH)的交角 此角代表合平面的斜度;此角越大代表合平面越陡,为安氏Ⅱ类面型倾向;反之此角越小代表合平面越平,为安氏Ⅲ类面型倾向 U1-SN角 上中切牙长轴与SN平面相交的下内角 反映上切牙对于前颅底的相对斜度;此角过大表示上颌中切牙唇倾,反之为舌倾 L1-MP角 下中切牙长轴与MP平面相交的上内角 反映下切牙对于下颌平面的倾斜度;此角过大表示下颌中切牙唇倾,反之为舌倾 上下中切牙角 上中切牙长轴与下中切牙长轴的交角 反映上下中切牙特别是上下前部牙弓的突度;此角越小突度越大,反之突度越小  下载: 导出CSV
下载: 导出CSV
表 2 4组一般资料的比较
X±S 一般资料 A组(n=49) B组(n=52) C组(n=50) 对照组(n=45) t/χ2 P 年龄/岁 6.33±1.26 6.29±1.22 6.32±1.25 6.31±1.11 0.01 0.998 身高/cm 106.33±2.11 105.69±2.30 105.89±2.13 106.74±2.22 2.19 0.090 BMI/(kg/m2) 19.98±1.46 20.05±1.22 19.88±1.52 20.56±1.45 2.47 0.088 性别/例(%) 2.019 0.568 男 29(59.18) 33(63.46) 25(50.00) 25(55.55) 女 20(40.81) 19(36.53) 25(50.00) 20(44.45) 头围/cm 51.33±1.36 51.13±1.69 50.99±1.58 51.46±1.58 0.86 0.464
下载: 导出CSV
表 3 4组声反射鼻咽腔测量参数比较
X±S 组别 例数 NAR/(cmH2O/L·min) NPV/cm3 A组 49 6.66±3.451)2) 16.44±6.121)2) B组 52 5.39±4.261)2) 15.46±5.121)2) C组 50 8.32±4.221) 13.52±4.331) 对照组 45 2.06±1.22 22.46±5.01 t 20.08 25.80 P < 0.001 < 0.001 与对照组比较,1) P < 0.05;与C组比较,2) P < 0.05。
下载: 导出CSV
表 4 4组头影参数比较
X±S 头影参数 A组(n=49) B组(n=52) C组(n=50) 对照组(n=45) F P SNA角 77.63±3.12 78.22±2.96 78.45±2.45 77.38±3.16 1.39 0.245 SNB角 74.13±2.151) 76.45±2.852) 78.92±3.461)2)3) 75.66±2.49 25.40 < 0.001 MP-FH角 34.22±4.261) 30.15±5.62 38.99±5.221)2)3) 28.56±4.05 44.78 < 0.001 NP-FH角 79.42±2.951) 83.45±3.662) 87.62±3.241)2)3) 84.27±3.52 49.88 < 0.001 Y轴角 67.59±3.281) 66.68±3.41 69.48±3.691)2)3) 65.49±3.51 4.49 < 0.001 OP-FH角 18.66±5.44 15.88±5.212) 20.36±4.682)3) 16.45±4.38 3.85 < 0.001 U1-SN角 80.95±6.861) 85.46±7.562) 88.76±4.661)2)3) 85.44±8.92 16.04 < 0.001 L1-MP角 86.79±7.01 89.25±8.45 88.49±6.99 89.11±9.26 0.99 0.400 上下中切牙角 143.62±11.68 137.45±12.64 149.86±15.421)2)3) 142.01±14.33 7.25 < 0.001 与对照组比较,1) P < 0.05;与A组比较,2) P < 0.05;与B组比较,3) P < 0.05。
下载: 导出CSV
表 5 3组间安氏Ⅱ类、Ⅲ类发生率比较
例(%) A组 B组 C组 安氏Ⅰ类 20a(40.8) 19a(36.5) 6b(12.0) 安氏Ⅱ类 24a(49.0) 6b(11.5) 20a(40.0) 安氏Ⅲ类 5a(10.2) 27b(51.9) 24b(48.0) a,b表示在0.05层次上2组间比较差异无统计学意义。
下载: 导出CSV
-
[1] 黄振云, 刘大波, 钟华敏, 等. 睡眠呼吸障碍儿童扁桃体及腺样体组织细菌学分析[J]. 中国耳鼻咽喉头颈外科, 2017, 24(3): 116-119. doi: 10.16066/j.1672-7002.2017.03.002
[2] 赵婷婷, 贺红. 儿童口呼吸与错畸形[J]. 中华口腔正畸学杂志, 2019, 26(4): 195-198. https://www.cnki.com.cn/Article/CJFDTOTAL-ZSKQ201908013.htm
[3] 于倩, 朱妍菲, 孙蕙珺, 等. 腺样体和/或扁桃体肥大相关替牙期骨性Ⅱ类儿童颌面部特点研究[J]. 中华口腔正畸学杂志, 2019, 26(4): 183-188.
[4] Elif B, Bahar GD, Ovsen O, et al. Oral health status of children with mouth breathing due to adenotonsillar hypertrophy[J]. Int J Pediatr Otorhinolaryngol, 2018, 113: 11-15. doi: 10.1016/j.ijporl.2018.07.018
[5] Fraga WS, Seixas VM, Santos JC, et al. Mouth breathing in children and its impact in dental malocclusion: a systematic review of observational studies[J]. Minerva Stomatol, 2018, 67(3): 129-138.
[6] Huang CC, Wu PW, Chen CL, et al. IL-17A expression in the adenoid tissue from children with sleep disordered breathing and its association with pneumococcal carriage[J]. Sci Rep, 2018, 8(1): 16770. doi: 10.1038/s41598-018-35169-x
[7] 崔佳文, 顾非, 王怡超, 等. 腺样体肥大检测手段的进展和评价[J]. 中国医药导报, 2020, 17(13): 62-65. https://www.cnki.com.cn/Article/CJFDTOTAL-YYCY202013016.htm
[8] 高淑蔚, 郭永丽, 许志飞. 阻塞性睡眠呼吸暂停综合征儿童腺样体扁桃体切除术后治疗效果及其预测因素的研究进展[J]. 中华耳鼻咽喉头颈外科杂志, 2020, 55(6): 630-634. doi: 10.3760/cma.j.cn115330-20191105-00666
[9] 杨菁菁, 程丽宇, 徐文. 儿童腺样体及扁桃体切除术后发音特征变化的研究[J]. 中华耳鼻咽喉头颈外科杂志, 2021, 56(7): 724-729.
[10] 李龙巧, 王胜国, 史先萍, 等. 内镜下行腺样体扁桃体切除术治疗儿童阻塞性睡眠呼吸暂停低通气综合征的疗效观察[J]. 河北医学, 2019, 25(8): 1308-1312. https://www.cnki.com.cn/Article/CJFDTOTAL-HCYX201908020.htm
[11] Milanesi JM, Pasinato F, Berwig LC, et al. Body posture and pulmonary function in mouth and nose breathing children: cross-sectional study[J]. Fisioter Mov, 2017, 30(1): 115-123. doi: 10.1590/1980-5918.030.001.ao12
[12] 陈文欣, 曹伟, 沈佳华, 等. OM85-BV对反复上呼吸道感染伴腺样体肥大的疗效及治疗机制初步探讨[J]. 临床耳鼻咽喉头颈外科杂志, 2020, 34(6): 499-504. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH202006005.htm
[13] 熊升华, 黄从付, 杨贵, 等. 两种不同方法治疗儿童腺样体肥大的临床对照研究[J]. 儿科药学杂志, 2020, 26(10): 29-32. https://www.cnki.com.cn/Article/CJFDTOTAL-EKYX202010011.htm
[14] Calvin J, Budiardjo SB, Setyanto DB, et al. Head Posture and Facial Profile of Mouth Breathing Children Caused by Nasal Obstruction[J]. Journal of International Dental and Medical Research, 2017, 10: 594-599.
[15] 张亚秋, 祁祎喆, 刘珂, 等. 腺样体肥大与牙颌面畸形的相关性研究[J]. 实用口腔医学杂志, 2017, 33(2): 215-218. https://www.cnki.com.cn/Article/CJFDTOTAL-SYKQ201702020.htm
[16] 杨凯, 曾祥龙, 俞梦孙. 口呼吸与鼻呼吸儿童颅面形态差异的研究[J]. 中华口腔医学杂志, 2002, 37(5): 385-387. https://www.cnki.com.cn/Article/CJFDTOTAL-ZHKY200205029.htm
[17] 贾曼玉, 邹世桢, 李进让. 儿童腺样体扁桃体肥大与肥胖相关性研究[J]. 中华耳鼻咽喉头颈外科杂志, 2020, 55(8): 760-763. https://cdmd.cnki.com.cn/Article/CDMD-10486-1020966588.htm
[18] 唐洁. 腺样体肥大与扁桃体肥大引起的气道狭窄对颅颌面结构生长发育影响的差异[J]. 健康之友, 2019, 30(21): 67-67.
[19] 黄振云, 刘大波, 钟华敏, 等. 睡眠呼吸障碍儿童扁桃体及腺样体组织细菌学分析[J]. 中国耳鼻咽喉头颈外科, 2017, 24(3): 116-119. https://www.cnki.com.cn/Article/CJFDTOTAL-EBYT201703002.htm
[20] 柳荫, 杨娜. 腺样体肥大并发分泌性中耳炎儿童的淋巴细胞亚群分布[J]. 实用医学杂志, 2017, 33(14): 2376-2379. https://www.cnki.com.cn/Article/CJFDTOTAL-SYYZ201714037.htm
[21] 杨凯, 曾祥龙, 俞梦孙. 儿童呼吸方式与颅面、气道、牙
[22] Jain A, Sahni JK. Polysomnographic studies in children undergoing adenoidectomy and / or tonsillectomy[J]. J Laryngol Otol, 2002, 116(9): 711-715.
[23] Deng J, Gao X. A case-control study of craniofacial features of children with obstructed sleep apnea[J]. Sleep Breath, 2012, 16(4): 1219-1227.
[24] Souki MQ, Soukj BQ, Franco LP, eI a1. Reliahility of subjective, linear, ratio and area cephalometric measurements in assessjng adenoid hypertrophy among different age grous[J]. Angle Orthod, 2012, 82(6): 1001-1007.
-
图(3)
表(5)
计量
- 文章访问数: 691
- PDF下载数: 128
- 施引文献: 0