
Diagnosis and treatment of 12 patients with deep neck infection and inferior mediastinal infection
-
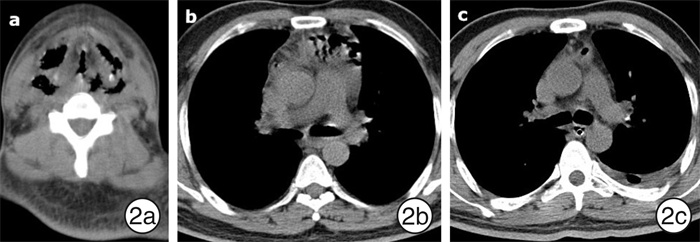
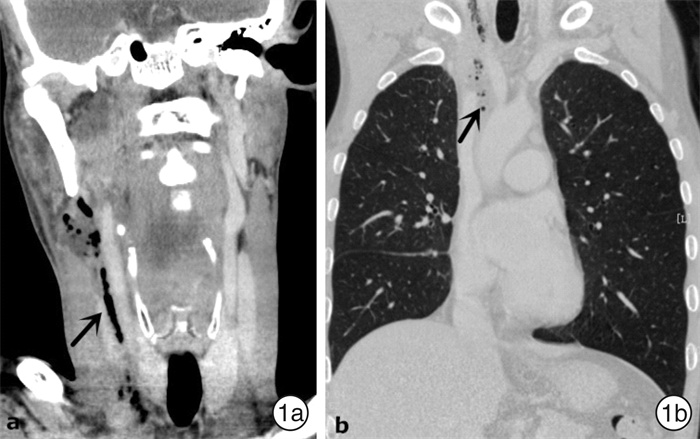
摘要: 目的 总结颈深部并下行性纵隔感染患者的临床表现和治疗治验。 方法 回顾12例颈深部并下行性纵隔感染患者的临床资料,分析临床表现、感染起源、细菌培养结果、相关系统疾病、手术引流方式及治疗结果。 结果 临床提示下行性纵隔感染典型表现为胸部疼痛,皮下捻发感。CT见颈部和纵隔积气及脓肿可确诊。感染起源主要为咽部感染,其次为牙源性感染。系统性疾病主要为糖尿病。术中取脓性分泌物培养,阳性率为58.3%(7/12),以链球菌感染为主。手术治疗包括9例单纯经颈部手术和3例颈胸部联合手术,胸部引流由胸外科通过胸腔镜、纵隔镜或B超引导下穿刺完成,无患者行开放手术。10例患者治愈,2例死亡,死亡率16.7%。 结论 颈深部并下行性纵隔感染早期无特异性,临床需提高警惕,以免延误诊治。及时的脓肿引流、有效的气道保护、抗菌治疗和处理潜在的危及生命的并发症是治疗成功的关键。Abstract: Objective To summarize the clinical manifestations and treatment of patients with deep neck infection with descending mediastinal infection. Methods The clinical data of 12 patients with deep neck infection with descending mediastinal infection were reviewed. The clinical manifestations, infection origin, bacterial culture results, related systemic diseases, surgical drainage methods and treatment results were analyzed. Results The typical clinical features of descending mediastinal infection were chest pain and subcutaneous crackling, diagnosis can confirmed by CT scan detected gas and abscess in the neck and mediastinal space. The main origin of infection was pharyngeal infection, followed by odontogenic infection. Systemic diseases were mainly diabetes mellitus. The positive rate of purulent secretion culture was 58.3%(7/12), streptococcus account for the highest proportion. Surgical treatment included 9 patients undergoing neck surgery alone and 3 patients undergoing combined neck and chest surgery. Chest drainage was performed by thoracic surgery through mediastinoscopy or thoracoscopic surgery or B-ultrasound guided puncture, and no patient underwent open surgery. Ten patients were cured and two died, with a mortality rate of 16.7%. Conclusion The deep neck infection with descending mediastinal infection has no specificity in the early stage. Timely abscess drainage, effective airway protection, antimicrobial therapy, and management of potentially life-threatening complications such as sepsis, mediastinitis, and pneumonia are the key to successful treatment.
-
Key words:
- deep neck infection /
- mediastinitis /
- diagnosis /
- therapy
-

-
表 1 12例颈部感染并DNM患者术前、术后感染指标比较
时间 白细胞/(×109·L-1) 中性粒细胞/(×109·L-1) NLR CRP/(mg·L-1) 术前 17.95±3.80 14.86±3.51 18.75±5.36 166.87±37.94 术后2 d 13.09±2.06 10.09±3.14 11.46±2.41 108.21±30.23 t 3.90 2.91 4.29 4.18 P 0.01 0.008 < 0.01 < 0.01 NLR:中性粒细胞百分比/淋巴细胞百分比率。  下载: 导出CSV
下载: 导出CSV
-
[1] Prado-Calleros HM, Jiménez-Fuentes E, Jiménez-Escobar I. Descending necrotizing mediastinitis: Systematic review on its treatment in the last 6 years, 75 years after its description[J]. Head Neck, 2016, 38 Suppl 1: E2275-E2283.
[2] Endo S, Murayama F, Hasegawa T, et al. Guideline of surgical management based on diffusion of descending necrotizing mediastinitis[J]. Jpn J Thorac Cardiovasc Surg, 1999, 47(1): 14-19.
[3] Wei D, Bi L, Zhu H, et al. Less invasive management of deep neck infection and descending necrotizing mediastinitis: A single-center retrospective study[J]. Medicine(Baltimore), 2017, 96(15): e6590.
[4] Kimura A, Miyamoto S, Yamashita T. Clinical predictors of descending necrotizing mediastinitis after deep neck infections[J]. Laryngoscope, 2020, 130(11): E567-E572.
[5] Petitpas F, Blancal JP, Mateo J, et al. Factors associated with the mediastinal spread of cervical necrotizing fasciitis[J]. Ann Thorac Surg, 2012, 93(1): 234-238. doi: 10.1016/j.athoracsur.2011.09.012
[6] 吴亚东, 赵科, 尹鑫海, 等. 口腔颌面颈部感染致坏死性纵隔炎5例[J]. 贵阳医学院学报, 2013, 38(5): 562, 564. https://www.cnki.com.cn/Article/CJFDTOTAL-GYYB201305045.htm
[7] Kimura A, Miyamoto S, Yamashita T. Clinical predictors of descending necrotizing mediastinitis after deep neck infections[J]. Laryngoscope, 2020, 130(11): E567-E572.
[8] 周兰柱, 周恩晖, 刘素茹, 等. 颈部坏死性筋膜炎的临床特点及处理策略[J]. 临床耳鼻咽喉头颈外科杂志, 2019, 33(6): 545-548. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH201906019.htm
[9] 葛鑫颖, 刘良发, 路承, 等. 食管异物穿孔致颈深间隙感染及纵隔脓肿的诊治[J]. 临床耳鼻咽喉头颈外科杂志, 2018, 32(4): 292-294. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH201804012.htm
[10] Sakai T, Matsutani N, Ito K, et al. Deep cervical and paratracheal drainage for descending necrotizing mediastinitis[J]. Asian Cardiovasc Thorac Ann, 2020, 28(1): 29-32. doi: 10.1177/0218492319896515
[11] Hsu RF, Wu PY, Ho CK. Transcervical drainage for descending necrotizing mediastinitis may be sufficient[J]. Otolaryngol Head Neck Surg, 2011, 145(5): 742-747. doi: 10.1177/0194599811406064
[12] Liew YT, Lim EY, Zulkiflee AB, et al. Severe descending necrotizing mediastinitis: vacuum-assisted dressing did wonder[J]. Gen Thorac Cardiovasc Surg, 2017, 65(4): 225-228. doi: 10.1007/s11748-016-0642-3
[13] 朱志超, 杨旭, 郑峰, 等. 颈部双平行切口联合纵隔镜或胸腔镜治疗颈部坏死性筋膜炎伴下行性坏死性纵隔炎的临床初探[J]. 中华口腔医学杂志, 2019, 54(5): 309-314. doi: 10.3760/cma.j.issn.1002-0098.2019.05.004
[14] Palma DM, Giuliano S, Cracchiolo AN, et al. Clinical features and outcome of patients with descending necrotizing mediastinitis: prospective analysis of 34 cases[J]. Infection, 2016, 44(1): 77-84. doi: 10.1007/s15010-015-0838-y
-
图(2)
表(1)
计量
- 文章访问数: 1071
- PDF下载数: 428
- 施引文献: 0