
-
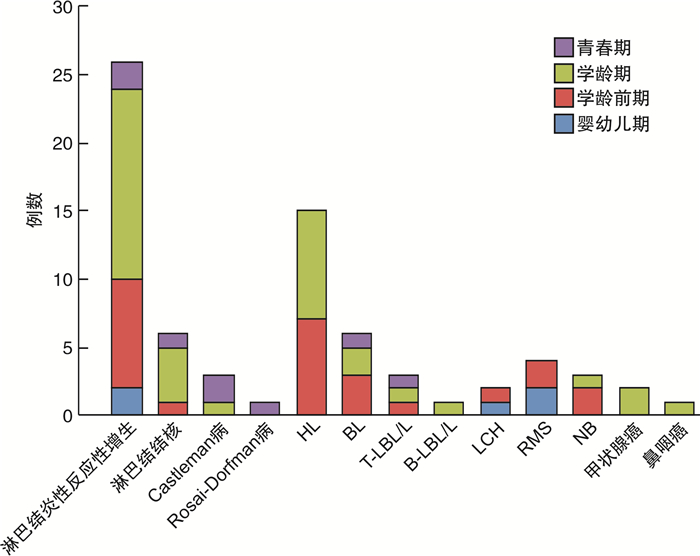
摘要: 目的 探讨不同病理类型的儿童颈部淋巴结病变的临床特征,为疾病的早期诊断提供帮助。方法 收集经淋巴结活检确诊的73例颈部淋巴结病变的患儿资料,分析不同病理类型的颈部淋巴结病变患儿的性别构成、年龄分布、淋巴结特征及临床表现。结果 73例颈部淋巴结病变患儿中,良性疾病组男性发病小于女性,恶性疾病组男性发病大于女性,两组性别构成差异均有统计学意义(P < 0.05)。良性疾病组在学龄期占比最大(27.4%),恶性疾病组在学龄前期(21.9%)和学龄期(20.5%)占比大,两组均在婴幼儿期和青春期占比较小,两组组内年龄分布差异有统计学意义(P < 0.01)。各病理类型中,73例患儿以淋巴结炎性反应性增生占比最大,为35.6%(26/73),主要在学龄期发病;其次为霍奇金淋巴瘤,占比20.5%(15/73),主要在学龄前期和学龄期发病。恶性疾病组的淋巴结平均最大横径值大于良性疾病组(P < 0.05)。良性疾病组的淋巴结主要分布于Ⅰ、Ⅱ、Ⅲ区,恶性疾病组的淋巴结主要分布于Ⅱ、Ⅲ、Ⅳ、Ⅴ区,两组间肿大淋巴结的分布差异有统计学意义(P < 0.01)。结论 不同病理类型的儿童颈部淋巴结病变在性别构成、年龄分布、淋巴结大小及分布上存在差异,儿童颈部淋巴结病变有其自身特点。Abstract: Objective Explore the clinical features of cervical lymph node lesions in children with different pathological types, and provide help for the early diagnosis of the disease.Method The data of 73 children with cervical lymph node disease diagnosed by lymph node biopsy were collected, and the gender composition, age distribution, lymph node characteristics and clinical manifestations of children with different pathological types were analyzed.Result Among the 73 children with cervical lymph node disease, the incidence of male patients in the benign disease group was less than that of female ones, and the incidence of male patients in the malignant disease group was greater than that of female ones, the difference in gender composition between the two groups was statistically significant(P < 0.05). The benign disease group had the largest proportion in the school-age period(27.4%), and the malignant disease group had a larger proportion in the preschool period(21.9%) and school-age period(20.5%), both groups had a relatively smaller proportion in the infant and adolescent period, the difference in age distribution within the group was statistically significant(P < 0.01). Among the various pathological types, the proportion of 73 children with lymph node inflammatory reactive hyperplasia was the largest, 35.6%(26/73), and was mainly at school age; the second was Hodgkin's lymphoma, accounting for 20.5%(15/73), mainly in the preschool and school age. The average maximum transverse diameter of lymph nodes in the malignant disease group was greater than that in the benign disease group(P < 0.05). The lymph nodes in the benign disease group were mainly distributed in areas Ⅰ, Ⅱ, and Ⅲ, and the lymph nodes in the malignant disease group were mainly distributed in areas Ⅱ, Ⅲ, Ⅳ, and Ⅴ, there was a statistically significant difference in the distribution of enlarged lymph nodes between the two groups(P < 0.01).Conclusion Different pathological types of cervical lymph node lesions in children are different in gender composition, age distribution, lymph node size and distribution, and cervical lymph node lesions in children have their own characteristics.
-
Key words:
- child /
- neck /
- lymphadenopathy /
- pathology
-

-
表 1 不同疾病组患儿的年龄总体分布
例(%) 组别 婴幼儿期 学龄前期 学龄期 青春期 χ2 P 良性疾病组 2(2.7) 9(12.3) 20(27.4) 5(6.8) 20.667 <0.01 恶性疾病组 3(4.1) 16(21.9) 15(20.5) 3(4.1) 16.946 <0.01 合计 5(6.8) 25(34.2) 35(47.9) 8(11.0) 33.247 <0.01  下载: 导出CSV
下载: 导出CSV
表 2 不同病理类型患儿肿大淋巴结的分布
例(%) 组别 例数 肿大淋巴结的分布 χ2 P Ⅰ区 Ⅱ区 Ⅲ区 Ⅳ区 Ⅴ区 Ⅵ区 良性疾病组 36 18(50.0) 32(88.9) 25(69.4) 13(36.1) 13(36.1) 7(19.4) 18.553 0.002 恶性疾病组 37 7(18.9) 29(78.4) 29(78.4) 35(94.6) 27(73.0) 14(37.8)
下载: 导出CSV
-
[1] 宋树林, 曾自三. 颈部常见淋巴结病的CT及MRI研究现状[J]. 中国中西医结合影像学杂志, 2019, 17(2): 212-214. https://www.cnki.com.cn/Article/CJFDTOTAL-JHYX201902034.htm
[2] Olu-eddo AN, Omoti CE. Diagnostic evaluation of primary cervical adenopathies in a developing country[J]. Pan Afr Med J, 2011, 10: 52. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3290882/
[3] Nolder AR. Paediatric cervical lymphadenopathy: when to biopsy?[J]. Curr Opin Otolaryngol Head Neck Surg, 2013, 21(6): 567-570. doi: 10.1097/MOO.0000000000000003
[4] Weinstock MS, Patel NA, Smith LP. Pediatric Cervical Lymphadenopathy[J]. Pediatr Rev, 2018, 39(9): 433-443. doi: 10.1542/pir.2017-0249
[5] Locke R, MacGregor F, Kubba H. The validation of an algorithm for the management of paediatric cervical lymphadenopathy[J]. Int J Pediatr Otorhinolaryngol, 2016, 81: 5-9. doi: 10.1016/j.ijporl.2015.11.034
[6] Wang J, Pei G, Yan J, et al. Unexplained cervical lymphadenopathy in children: predictive factors for malignancy[J]. J Pediatr Surg, 2010, 45(4): 784-788. doi: 10.1016/j.jpedsurg.2009.08.018
[7] Citak EC, Koku N, Demirci M, et al. A retrospective chart review of evaluation of the cervical lymphadenopathies in children[J]. Auris Nasus Larynx, 2011, 38(5): 618-621. doi: 10.1016/j.anl.2011.01.009
[8] Ludwig BJ, Wang J, Nadgir RN, et al. Imaging of cervical lymphadenopathy in children and young adults[J]. AJR Am J Roentgenol, 2012, 199(5): 1105-1113. doi: 10.2214/AJR.12.8629
[9] Celenk F, Baysal E, Aytac I, et al. Incidence and predictors of malignancy in children with persistent cervical lymphadenopathy[J]. Int J Pediatr Otorhinolaryngol, 2013, 77(12): 2004-2007. doi: 10.1016/j.ijporl.2013.09.022
[10] Rajasekaran K, Krakovitz P. Enlarged neck lymph nodes in children[J]. Pediatr Clin North Am, 2013, 60(4): 923-936. doi: 10.1016/j.pcl.2013.04.005
[11] Rosenberg TL, Nolder AR. Pediatric cervical lymphadenopathy[J]. Otolaryngol Clin North Am, 2014, 47(5): 721-731.
-
图(1)
表(2)
计量
- 文章访问数: 1095
- PDF下载数: 1254
- 施引文献: 0