
Clinical analysis of 12 cases of solitary fibrous tumors in nasal cavity, sinuses and skull base
-
摘要: 目的 总结分析鼻腔鼻窦颅底孤立性纤维性肿瘤(solitary fibrous tumor,SFT)的临床表现、诊疗方法及预后特点。方法 回顾性分析青岛大学附属医院耳鼻咽喉头颈外科和颅底外科2014年4月-2022年1月收治的12例鼻腔鼻窦颅底SFT患者的临床资料,其中耳鼻咽喉头颈外科收治患者4例、颅底外科收治患者8例,分析其临床特点、诊疗经过及预后情况。患者均行手术治疗,其中4例术后辅助放化疗,8例未行放化疗。结果 术后随访12~60个月,4例术后辅助放化疗的患者均预后良好;8例未行放化疗患者中6例预后良好,另2例复发;4例患者既往有SFT手术史,复发后收治于青岛大学附属医院治疗,其中1例术后复发。所有患者均无转移。结论 鼻腔鼻窦颅底SFT较为罕见,对于该病最有效的治疗手段为手术切除,术后辅助放化疗及术后长期随访可以实现较好的预后。综合治疗中完整性手术切除肿瘤是治疗的关键。Abstract: Objective To summarize and analyze the clinical manifestations, diagnosis and management and prognostic features of solitary fibrous tumor(SFT) in nasal cavity, sinus and skull base.Methods The clinical data of 12 patients with STF from nasal cavity, sinus and cranial base admitted to the Affiliated Hospital of Qingdao University from April 2014 to January 2022 were retrospectively analyzed, including 4 patients admitted to the department of Otolaryngology head and neck surgery and 8 patients admitted to the department of skull base surgery The clinical characteristics, diagnosis, management and prognosis were analyzed.Results Twelve patients were included in this research, including 7 males and 5 females. All patients received surgical treatment, and 4 patients also received postoperative adjuvant chemoradiotherapy. After follow-up for 12-60 months, 4 patients with adjuvant radiotherapy and chemotherapy had a good prognosis, and among 8 patients who did not receive radiotherapy and chemotherapy, 6 patients had good prognosis and 2 patients showed relapse. Four patients with a history of recurrence of SFT after surgery were admitted to our hospital for surgical treatment, in which 1 patient had relapse after surgery, and none had metastasis. Nasal cavity and sinus to skull base SFT is rare. The most effective treatment for this disease is surgical resection, and postoperative adjuvant chemoradiation and long-term follow-up can achieve a better prognosis. En bloc resection is the key to treatment success.
-
Key words:
- nasal and sinus tumors /
- basicranial tumor /
- solitary fibrous tumor
-

-
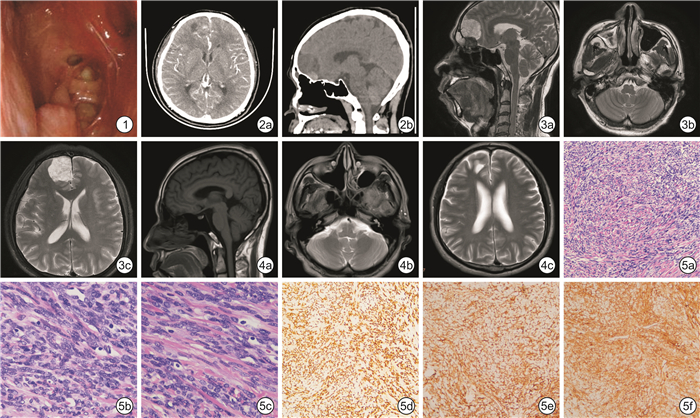
图 1 术前电子纤维喉镜 右侧鼻腔呈术后改变,可见脓涕倒流,咽鼓管口通畅,咽隐窝、鼻咽顶后壁无新生物;图2 术前颅脑CT检查 2a:失状位;2b:轴位;右侧额叶可见团块状高低混杂密度影,边界欠清;图3 术前颅脑MRI平扫所见 3a:失状位;3b:轴位(鼻腔鼻窦平面);3c:轴位(额叶平面);右侧额叶可见团块状不均匀信号影,长径约30 mm,内部似见分隔,边界清晰;图4 术后22个月颅脑MRI平扫所见 4a:失状位;4b:轴位(鼻腔鼻窦平面);4c:轴位(额叶平面);恢复良好无复发,符合鼻窦术后改变。图5 术后病理检查 镜下见大量梭形及卵圆形细胞,结合免疫学表型特征,符合SFT(中间性肿瘤);5a:苏木精-伊红染色×10;5b、5c:苏木精-伊红染色×40;5d:STAT6染色×10;5e:CD99染色×10;5f:CD34染色×10。
表 1 12例鼻腔鼻窦颅底SFT患者临床资料
例序 年龄/岁 性别 临床表现 病变特点及范围 出血量/ mL 病理组化 放疗 预后 1 57 男 鼻塞、嗅觉减退、头痛、头晕 位于右侧额叶,局部与脑组织粘连,血供丰富 300 STAT6(+)、CD99(+)、CD34(+)、CK(-)、S-100(-)、SMA(-)、Desmin(-)、Ki-67阳性率约5% 是 随访22个月无复发 2 71 男 鼻塞、嗅觉减退 位于鼻中隔后端,局部突入鞍区,包绕颈内动脉,硬脑膜欠完整,呈分叶状,质韧,血供丰富 100 CD34(+)、CD99(+)、STAT6(+)、S-100(-)、SMA(-)、EMA(-)、Desmin(-)、Ki-67阳性率2% 是 随访18个月无复发 3 73 女 鼻塞、嗅觉减退、鼻出血 位于右侧筛顶,包膜完整,血供丰富 50 CD34(+)、CD99(+)、STAT6(+)、Vimentin(+)、CK(-)、Desmin(-)、SMA(-)、S-100(-)、Ki-67阳性率约10% 否 随访24个月无复发 4 24 女 鼻塞、嗅觉减退 位于左侧下鼻甲后端,包膜完整、血供丰富 50 STAT6(+)、CD34(+)、CD99(+)、S-100弱(+)、SMA(-)、Desmin(-)、Ki-67阳性率约5% 否 随访36个月无复发 5 53 女 面部麻木、眼睑下垂 位于海绵窦,有包膜,血供丰富 500 STAT6(+)、CD34(+)、CD99(+)、Vimentin(+)、S-100(-)、EMA(-)、PR(-)、Ki-67阳性率约10% 否 随访48个月无复发 6 63 男 头晕、头痛 位于左枕下,与横窦、乙状窦粘连,血供丰富 400 STAT6(+)、CD34部分(+)、CD99(+)、Vimentin(+)、EMA(-)、SMA(-)、S-100(-)、Desmin(-)、Ki-67阳性率约30% 是,加做化疗 9年前行颅后窝SFT手术。随访60个月无复发 7 82 男 突眼、眼球运动受限、视力丧失 位于左眶外侧壁,凸向颅底,挤压视神经,有包膜,血供丰富 120 STAT6(+)、CD34(+)、CD99(+)、Bcl-2(+)、PR(-)、EMA(-)、S-100(-)、Ki-67阳性率约30% 否 随访24个月,患者左眼眶肿瘤复发 8 62 男 突眼、视力下降 位于右眶外侧壁及上壁,挤压视神经,有包膜,血供丰富 80 STAT6(+)、CD34(+)、CD99(+)、Vimentin(+)、EMA局灶弱(+)、S-100(-)、Ki-67阳性率约20% 否 10年前行右侧眼眶SFT手术。随访55个月右眼眶肿瘤复发 9 37 女 视力下降、眼睑下垂、头痛 位于左侧海绵窦内,与三叉神经、眼神经、上颌神经、滑车神经粘连,质软,血供丰富 400 STAT6(+)、CD34(+)、CD99(+)、Vimentin(+)、Bcl-2(+)、S-100(-)、EMA(-)、Ki-67阳性率约10% 否 随访48个月无复发 10 56 男 头痛、视力下降 位于颅后窝,侵犯小脑膜,呈分叶状,有包膜,血供丰富 1 800 STAT6部分(+)、CD99(+)、Vimentin(+)、CD34(-)、EMA(-)、S-100(-)、Ki-67阳性率约5% 否 6年前行枕部SFT手术。随访28个月,患者无复发 11 62 男 头晕、眼睑下垂、鼻塞、嗅觉下降 位于左侧额叶,眶壁骨质缺损,有包膜,血供丰富 80 STAT6(+)、CD34部分(+)、CD99(+)、Vimentin(+)、SSTR2(-)、S-100(-)、Ki-67阳性率约3% 否 18年前行左侧额叶SFT手术。随访28个月无复发 12 33 女 头晕、鼻塞、嗅觉下降 位于额窦中线区,局部与脑组织粘连,呈分叶状,血供丰富 100 STAT6部分(+)、CD34(+)、CD99(+)、SSTR2(-)、PR(-)、S-100(-)、Ki-67阳性率约5% 是 随访12个月无复发  下载: 导出CSV
下载: 导出CSV
-
[1] Stout AP, Himadi GM, et al. Solitary(localized) mesothelioma of the pleura[J]. AnnSurg, 1951, 133(1): 50-64.
[2] 梁乐平, 赵倩倩, 张军军, 等. 经口机器人手术治疗喉下咽食管入口孤立性纤维性肿瘤1例并文献复习[J]. 临床耳鼻咽喉头颈外科杂志, 2024, 38(2): 168-171. 10.13201/j.issn.2096-7993.2024.02.017
[3] Machado I, Nieto Morales MG, Cruz J, et al. Solitary Fibrous Tumor: Integration of Clinical, Morphologic, Immunohistochemical and Molecular Findings in Risk Stratification and Classification May Better Predict Patient outcome[J]. Int J Mol Sci, 2021, 22(17): 9423. doi: 10.3390/ijms22179423
[4] Schöffski P, Timmermans I, Hompes D, et al. Clinical Presentation, Natural History, and Therapeutic Approach in Patients with Solitary Fibrous Tumor: A Retrospective Analysis[J]. Sarcoma, 2020, 2020: 1385978.
[5] 俞祯妮, 罗军德, 黄聪, 等. 头颈部孤立性纤维瘤的CT及MR分析[J]. 现代医用影像学, 2020, 29(6): 1020-1023. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYY202006011.htm
[6] Peng Z, Wang Y, Wang Y, et al. Hemangiopericytoma/solitary fibrous tumor of the cranial base: a case series and literature review[J]. BMC Surg, 2022, 22(1): 289. doi: 10.1186/s12893-022-01718-5
[7] Park HK, Yu DB, Sung M, et al. Molecular changes in solitary fibrous tumor progression[J]. J Mol Med(Berl), 2019, 97(10): 1413-1425.
[8] Robinson DR, Wu YM, Kalyana-Sundaram S, et al. Identification of recurrent NAB2-STAT6 gene fusions in solitary fibrous tumor by integrative sequencing[J]. Nat Genet, 2013, 45(2): 180-185. doi: 10.1038/ng.2509
[9] Smrke A, Thway K, H Huang P, et al. Solitary fibrous tumor: molecular hallmarks and treatment for a rare sarcoma[J]. Future Oncol, 2021, 17(27): 3627-3636. doi: 10.2217/fon-2021-0030
[10] Tariq MU, Din NU, Abdul-Ghafar J, et al. The many faces of solitary fibrous tumor; diversity of histological features, differential diagnosis and role of molecular studies and surrogate markers in avoiding misdiagnosis and predicting the behavior[J]. Diagn Pathol, 2021, 16(1): 32. doi: 10.1186/s13000-021-01095-2
[11] Lococo F, Cesario A, Mulè A, Margaritora S. Malignant solitary fibrous tumor of the esophagus[J]. Eur J Cardiothorac Surg, 2011, 39(4): 595-597. doi: 10.1016/j.ejcts.2010.07.031
[12] 林莉莉, 张妍, 宋洪涛, 等. 孤立性纤维性肿瘤晚期药物治疗研究进展[J]. 国际药学研究杂志, 2019, 46(1): 17-21. https://www.cnki.com.cn/Article/CJFDTOTAL-GWYZ201901005.htm
[13] Zhang K, Liu HJ, Cheng ZB, et al. Solitary fibrous tumor: a 10-year retrospective analysis with several rare cases[J]. Chin Med J(Engl), 2020, 134(8): 1006-1008.
[14] Machado I, Nieto-Morales G, Cruz J, et al. Controversial issues in soft tissue solitary fibrous tumors: A pathological and molecular review[J]. Pathol Int, 2020, 70(3): 129-139. doi: 10.1111/pin.12894
[15] 王明婕, 侯丽珍, 周兵, 等. 鼻腔鼻窦内翻性乳头状瘤恶变的相关危险因素分析[J]. 临床耳鼻咽喉头颈外科杂志, 2021, 35(7): 627-632. doi: 10.13201/j.issn.2096-7993.2021.07.011
-
计量
- 文章访问数: 108
- 施引文献: 0