
-
摘要: 目的 探讨IgG4相关疾病(IgG4-RD)的临床特征和影像学特征,提高鼻咽IgG4-RD早期的诊断能力,减少误诊与漏诊。方法 通过电子病例系统采集患者基本信息,包括年龄、性别、症状、病程和诊疗过程。记录患者住院期间及门诊随诊的实验室检查资料,包括鼻内镜检查、EB病毒水平、IgG4水平及C反应蛋白水平等。对患者的CT、MRI以及PET-CT特征进行总结分析,并收集所有患者的病理和免疫组织化学结果。结果 4例患者均行病灶部分切除活检术,病理结果显示炎性肉芽组织和纤维组织增生,淋巴细胞、浆细胞和中性粒细胞浸润较多,免疫组织化学IgG4+浆细胞每高倍视野均>10个。结合病史、影像学检查、血清学结果及相关治疗,最终诊断为IgG4-RD,经激素和免疫抑制治疗后症状均有明显改善。结论 IgG4-RD与鼻咽癌的临床表现高度相似,对伴有似鼻咽癌症状且多次活检无法明确病理的患者,需要与IgG4-RD进行鉴别,及时诊断IgG4-RD对预防活动性疾病患者继发性脏器损害具有重要意义。Abstract: Objective The purpose of this article was to discuss the clinical features and imaging characteristics of IgG4-related disease(IgG4-RD) in order to identify nasopharyngeal IgG4-RD at an early stage.Methods The basic information of the patients, including age, sex, symptoms, disease duration and treatment process, was collected through the electronic case system. Laboratory tests including nasal endoscopy, EBV levels, IgG4 levels and C-reactive protein levels were recorded during hospitalization and outpatient follow-up. All radiological imaging and postoperative pathology data are collected, analyzed and summarized.Results All patients underwent partial excisional biopsy of the lesion. The pathological findings showed inflammatory granulomatous and fibrous tissue hyperplasia with a high infiltration of lymphocytes, plasma cells and neutrophils, and immunohistochemistry examination showed IgG4+ plasma cells were more than 10 per high magnification field. Combining medical history, imaging, serological findings and relevant treatment, all four patients were diagnosed with IgG4-associated disease. And their symptoms improved significantly after hormonal and immunosuppressive treatment.Conclusion IgG4-RD has a highly similar clinical presentation with nasopharyngeal carcinoma. Differentiation from IgG4-RD should be considered for those pathology cannot be clarified by multiple biopsies. Timely diagnosis of IgG4-RD is important to prevent secondary organ damage in patients with active disease.
-
Key words:
- IgG4-related disease /
- nasopharyngeal neoplasms /
- rare diseases /
- diagnose
-

-
表 1 鼻咽部IgG4-RD患者基本情况
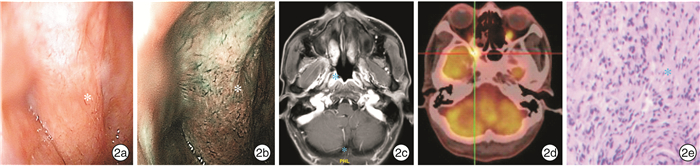
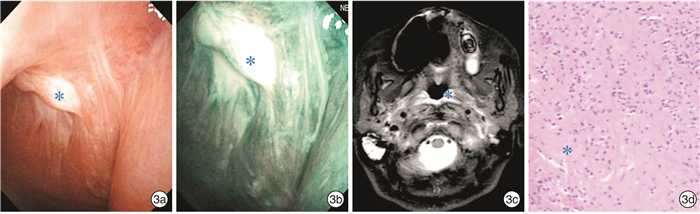
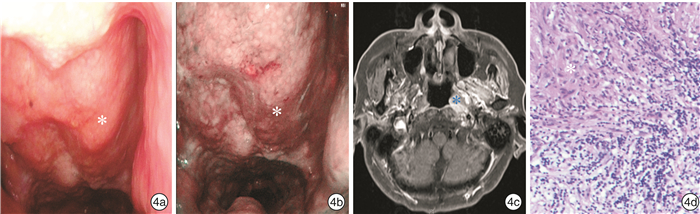
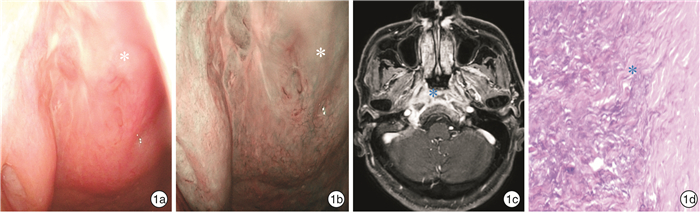
例序 性别 年龄/岁 病程 症状 EB病毒 血清IgG4/(mg·dL-1) IgG4+细胞/每高倍镜视野 治疗 转归 1 男 63 5个月 反复头痛 - 218 22 激素+环磷酰胺 缓解 2 男 53 5个月 鼻出血、复视 + 324 >10 激素+环磷酰胺 缓解 3 女 64 4个月 头痛 + 268 75 激素+环磷酰胺 缓解 4 男 66 6个月 头痛 - 765 >10 激素+环磷酰胺 缓解  下载: 导出CSV
下载: 导出CSV
-
[1] Shimizu Y, Yamamoto M, Naishiro Y, et al. Necessity of early intervention for IgG4-related disease-delayed treatment induces fibrosis progression[J]. Rheumatology(Oxford), 2013, 52(4): 679-683. doi: 10.1093/rheumatology/kes358
[2] Della-Torre E, Lanzillotta M, Doglioni C. Immunology of IgG4-related disease[J]. Clin Exp Immunol, 2015, 181(2): 191-206. doi: 10.1111/cei.12641
[3] Bledsoe JR, Della-Torre E, Rovati L, et al. IgG4-related disease: review of the histopathologic features, differential diagnosis, and therapeutic approach[J]. APMIS, 2018, 126(6): 459-476. doi: 10.1111/apm.12845
[4] Sasaki T, Takahashi K, Mineta M, et al. Immunoglobulin G4-related sclerosing disease mimicking invasive tumor in the nasal cavity and paranasal sinuses[J]. AJNR Am J Neuroradiol, 2012, 33(2): E19-20. doi: 10.3174/ajnr.A2495
[5] Völker HU, Scheich M, Zettl A, et al. Laryngeal inflammatory myofibroblastic tumors: Different clinical appearance and histomorphologic presentation of one entity[J]. Head Neck, 2010, 32(11): 1573-1578. doi: 10.1002/hed.21232
[6] Cho HK, Lee YJ, Chung JH, et al. Otologic Manifestation in IgG4-Related Systemic Disease[J]. Clin Exp Otorhinolaryngol, 2011, 4(1): 52-54. doi: 10.3342/ceo.2011.4.1.52
[7] Umehara H, Okazaki K, Masaki Y, et al. Comprehensive diagnostic criteria for IgG4-related disease(IgG4-RD), 2011[J]. Mod Rheumatol, 2012, 22(1): 21-30. doi: 10.3109/s10165-011-0571-z
[8] Kamisawa T, Zen Y, Pillai S, et al. IgG4-related disease[J]. Lancet, 2015, 385(9976): 1460-1471. doi: 10.1016/S0140-6736(14)60720-0
[9] Deshpande V, Zen Y, Chan JK, et al. Consensus statement on the pathology of IgG4-related disease[J]. Mod Pathol, 2012, 25(9): 1181-1192. doi: 10.1038/modpathol.2012.72
[10] Khosroshahi A, Wallace ZS, Crowe JL, et al. Second International Symposium on IgG4-Related Disease. International Consensus Guidance Statement on the Management and Treatment of IgG4-Related Disease[J]. Arthritis Rheumatol, 2015, 67(7): 1688-1699. doi: 10.1002/art.39132
[11] Takahashi H, Yamashita H, Morooka M, et al. The utility of FDG-PET/CT and other imaging techniques in the evaluation of IgG4-related disease[J]. Joint Bone Spine, 2014, 81(4): 331-336. doi: 10.1016/j.jbspin.2014.01.010
-
图(4)
表(1)
计量
- 文章访问数: 1059
- PDF下载数: 204
- 施引文献: 0