
-
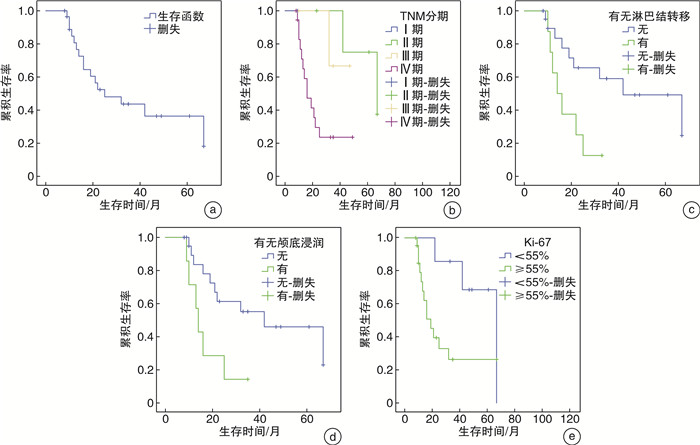
摘要: 目的 探讨鼻腔鼻窦神经内分泌癌(SNEC)的临床特点及影响预后的因素。方法 回顾性分析31例确诊为SNEC患者的临床资料。31例患者中,单纯手术切除3例,手术+放疗4例,手术+化疗4例,手术+放化疗10例,未行手术单纯放化疗10例。随访8~64个月。结果 至随访结束,2例患者失访,17例死亡,12例存活,8例复发,5年总生存率36.4%,高TNM分期、淋巴结转移、颅底浸润以及Ki-67≥55%是其预后不良因素。结论 SNEC是一种罕见的侵袭性肿瘤,预后差、局部复发率高、有转移倾向,且起病隐匿,手术联合放化疗的综合治疗仍是最佳的治疗方式。Abstract: Objective To investigate the characteristics and prognostic factors of sinonasal neuroendocrine carcinoma (SNEC).Methods The clinical data of 31 patients with SNEC were retrospectively analyzed. Among the 31 patients, 3 cases were simply surgically removed, 4 cases were surgery + radiotherapy, 4 cases were surgery + chemotherapy, 10 cases were surgery + chemoradiotherapy, and 10 cases were simply given chemoradiotherapy without surgery. The study follow-up 8-64 months.Results By the end of follow-up, 2 patients were lost to follow-up, 17 died, 12 survival, 8 relapsed and 5-year survival rate was 36.4%. High TNM stage, lymph node metastasis, skull base infiltration and Ki-67≥55% were the negative prognostic factors for survival.Conclusion SNEC is a rare aggressive tumor, with poor prognosis, high local recurrence rate, metastasis tendency, hidden disease. The comprehensive treatment of surgery combined with chemoradiotherapy is still the best treatment.
-
Key words:
- neuroendocrine carcinoma /
- nose neoplasms /
- prognosis
-

-
表 1 31例SNEC患者的一般资料
临床特征 例数(%) 临床特征 例数(%) 性别 首发症状 男 25(80.6) 鼻塞 22(71.0) 女 6(19.4) 鼻出血 13(41.9) 年龄/岁 头疼 12(38.7) < 50 12(38.7) 眼部胀痛 9(29.0) ≥50 19(61.3) 面部麻木 3(9.7) 肿瘤位置 TNM分期 左侧 15(48.4) Ⅰ期 1(3.2) 右侧 10(32.3) Ⅱ期 6(19.4) 双侧 6(19.4) Ⅲ期 5(16.1) 淋巴结转移 Ⅳ期 19(61.3) 有 8(25.8) 免疫组织化学 无 23(74.2) Ki-67/% 颅底浸润 < 55 7(22.6) 有 7(22.6) ≥55 24(77.4) 无 24(77.4) CK+ 29(93.5) 病理类型 Syn+ 30(96.8) 小细胞型 30(96.8) CD56+ 25(80.6) 大细胞型 1(3.2) CgA+ 8(25.8)  下载: 导出CSV
下载: 导出CSV
-
[1] Elisabeth HMM, Alvaro DM, Turker YM, et al. Multimodality treatment for sinonasal neuroendocrine carcinoma[J]. Head Neck, 2012, 34(10): 1372-1376. doi: 10.1002/hed.21940
[2] Patel TD, Vazquez A, Dubal PM, et al. Sinonasal neuroendocrine carcinoma: a population-based analysis of incidence and survival[J]. Int Forum Allergy Rhinol, 2015, 5(5): 448-453. doi: 10.1002/alr.21497
[3] Rindi G, Inzani F. Neuroendocrine neoplasm update: toward universal nomenclature[J]. Endocr Relat Cancer, 2020, 27(6): R211-R218. doi: 10.1530/ERC-20-0036
[4] Yao JC, Hassan M, Phan A, et al. One hundred years after "carcinoid": epidemiology of and prognostic factors for neuroendocrine tumors in 35, 825 cases in the United States[J]. J Clin Oncol, 2008, 26(18): 3063-3072. doi: 10.1200/JCO.2007.15.4377
[5] Rivero A, Liang J. Sinonasal small cell neuroendocrine carcinoma: a systematic review of 80 patients[J]. Int Forum Allergy Rhinol, 2016, 6(7): 744-751. doi: 10.1002/alr.21734
[6] 郑国峰, 应红芳, 周水洪. 头颈部神经内分泌癌[J]. 中华耳鼻咽喉头颈外科杂志, 2015, 50(3): 260-264. doi: 10.3760/cma.j.issn.1673-0860.2015.03.021
[7] 袁璇, 谢志海, 章华, 等. 鼻及颅底神经内分泌癌的临床特征及内镜手术切除疗效分析[J]. 临床耳鼻咽喉头颈外科杂志, 2021, 35(8): 740-745. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH202108014.htm
[8] 方三高, 魏建国, 周晓军. 解读WHO(2017)头颈部肿瘤分类(鼻腔、鼻窦、颅底)[J]. 诊断病理学杂志, 2018, 25(4): 241-245. doi: 10.3969/j.issn.1007-8096.2018.04.001
[9] Bell D, Hanna EY, Weber RS, et al. Neuroendocrine neoplasms of the sinonasal region[J]. Head Neck, 2016, 38 Suppl 1: E2259-2266. https://pubmed.ncbi.nlm.nih.gov/26041714/
[10] van der Laan TP, Iepsma R, Witjes MJ, et al. Meta-analysis of 701 published cases of sinonasal neuroendocrine carcinoma: The importance of differentiation grade in determining treatment strategy[J]. Oral Oncol, 2016, 63: 1-9. doi: 10.1016/j.oraloncology.2016.10.002
[11] Abdelmeguid AS, Bell D, Hanna EY. Neuroendocrine Carcinoma and Sinonasal Undifferentiated Carcinoma[J]. Adv Otorhinolaryngol, 2020, 84: 168-184. https://pubmed.ncbi.nlm.nih.gov/32731236/
[12] Wakasaki T, Yasumatsu R, Masuda M, et al. Small Cell Carcinoma in the Head and Neck[J]. Ann Otol Rhinol Laryngol, 2019, 128(11): 1006-1012. doi: 10.1177/0003489419853601
[13] Feola T, Centello R, Sesti F, et al. Neuroendocrine Carcinomas with Atypical Proliferation Index and Clinical Behavior: A Systematic Review[J]. Cancers(Basel), 2021, 13(6): 1247. https://pubmed.ncbi.nlm.nih.gov/33809007/
[14] Milione M, Maisonneuve P, Spada F, et al. The Clinicopathologic Heterogeneity of Grade 3 Gastroenteropancreatic Neuroendocrine Neoplasms: Morphological Differentiation and Proliferation Identify Different Prognostic Categories[J]. Neuroendocrinology, 2017, 104(1): 85-93. doi: 10.1159/000445165
[15] Sorbye H, Welin S, Langer SW, et al. Predictive and prognostic factors for treatment and survival in 305 patients with advanced gastrointestinal neuroendocrine carcinoma(WHO G3): the NORDIC NEC study[J]. Ann Oncol, 2013, 24(1): 152-160. doi: 10.1093/annonc/mds276
-
图(1)
表(1)
计量
- 文章访问数: 2435
- PDF下载数: 1180
- 施引文献: 0