
Difference of SLC26A4 gene mutation frequency between patients with large vestibular aqueduct syndrome and/or Mondini dysplasia
-
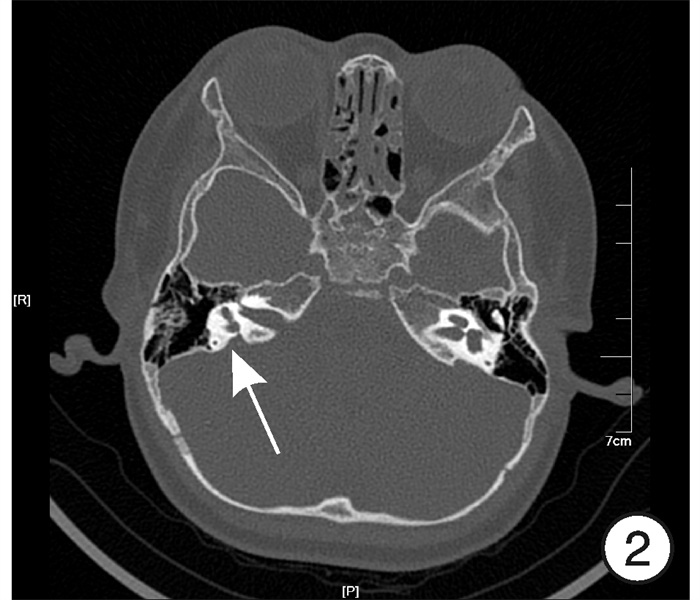
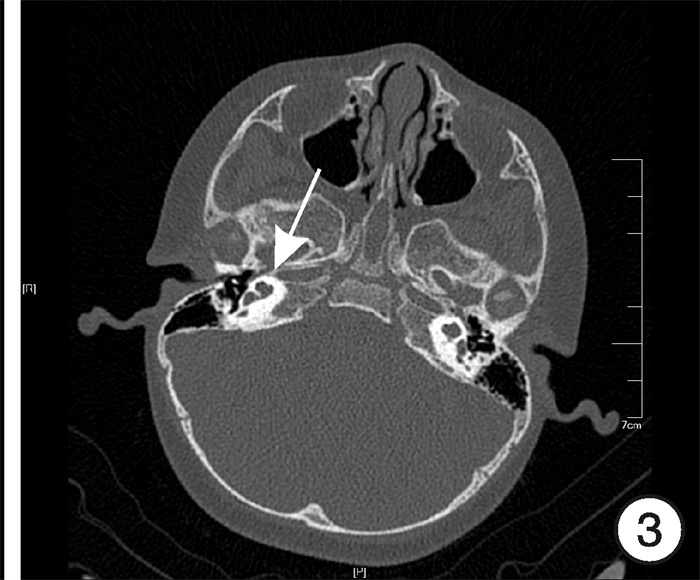
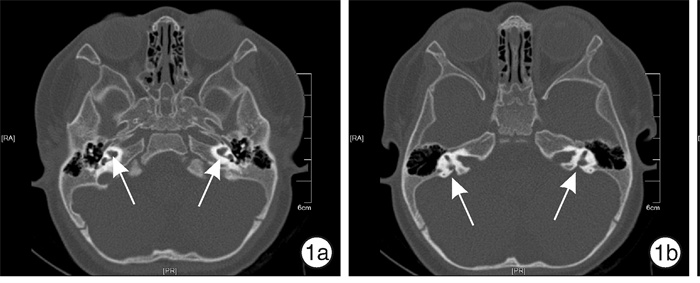
摘要: 目的 评估SLC26A4基因在大前庭水管综合征(EVAS)和/或Mondini畸形(MD)患儿中的突变频率, 为临床耳聋的分子诊断提供证据。方法 对74例患儿行颞骨薄层CT检查, 并进行二代测序, 分析SLC26A4基因编码的外显子。结果 共发现EVAS合并MD(E+M)37例, 单独EVAS(E)28例, 单独MD(M)9例。74例患儿中66例(89.2%)发现突变, 其中双等位基因突变64例(86.5%), 单等位基因突变2例(2.7%)。不同组的SLC26A4突变检出率差异有统计学意义(P < 0.001), M组突变发生率明显低于E组、E+M组(P < 0.001)。E组28例中发现SLC26A4双等位基因27例(96.4%), 单等位基因1例(3.6%); E+M组37例中发现SLC26A4双等位基因37例(100%); M组9例中只发现1例(11.1%)携带SLC26A4单杂合突变。结论 EVAS合并MD、单独EVAS与单独MD有着完全不同的发病机制, 早期EVAS和/或MD患儿的临床遗传学诊断有助于提供听力损失遗传原因的精确信息和遗传咨询, 从而实施适当的疾病控制和预防措施, 下一代测序技术在耳聋的分子诊断中发挥愈加重要的作用。Abstract: Objective The purpose of this study was to evaluate the mutation frequency of SLC26A4 gene in patients with enlarged vestibular aqueduct syndrome(EVAS) and/or Mondini dysplasia(MD), so as to provide evidence for molecular diagnosis of deafness.Methods In total, 74 patients with sensorineural hearing loss were included in this study. All patients underwent thin-layer CT examination of temporal bone. The coding exons of SLC26A4 were analyzed by second-generation sequencing in all subjects.Results Among them, 37 patients with EVAS and MD(E+M group), 28 patients with EVAS and without MD(E group), and 9 patients with isolated MD(M group) were identified. In 74 cases, 66 cases(89.2%) were found to have mutation, including 64 cases(86.5%) of biallelic mutation and two cases(2.7%) of single allele mutation. The detection rate of SLC26A4 in different groups was statistically significant(P < 0.001). The mutation rate in group M was significantly lower than that in Group E and E+M(P < 0.001). In Group E, 27 cases(96.4%) had SLC26A4 biallelic mutations and one case(3.6%) had SLC26A4 single allele mutation, respectively; in Group E+M, 37 cases(100%) had SLC26A4 biallelic mutations; in group M, only one patient(11.1%) carried monoallelic mutations of the SLC26A4 gene.Conclusion There are totally different pathogenesis in Chinese EVAS patients with or without MD, or isolated MD. Early clinical genetic diagnosis of patients with EVAS and/or MD helps to provide accurate information about the genetic causes of hearing loss, provide genetic counseling, and implement appropriate disease control and prevention measures. Next generation sequencing technology plays an increasingly important role in molecular diagnosis of deafness.
-

-
表 2 SLC26A4基因的突变谱和发生频率
畸形 基因型 氨基酸 发生频率/例(%) 单独EVAS c.919-2A>G/c.919-2A>G 剪切位点 9(32.1) c.919-2A>G/c.2168A>G 剪切位点/H723R 4(14.3) c.919-2A>G/c.1174A>T 剪切位点/N392Y 2(7.1) c.919-2A>G/c.ivs15+5G>A 剪切位点 1(3.6) c.919-2A>G/c.1079C>T 剪切位点/A360V 1(3.6) c.919-2A>G/c.1226G>A 剪切位点/R409H 1(3.6) c.919-2A>G/c.1229C>T 剪切位点/T410M 1(3.6) c.919-2A>G/589G>A 剪切位点/G197R 1(3.6) c.919-2 A>G/c.1586T>G 剪切位点/I529S 1(3.6) c.919-2 A>G/c.1262A>C 剪切位点/Q421P 1(3.6) c.919-2 A>G/c.1318A>T 剪切位点/K440X 1(3.6) c.919-2 A>G/c.1975G>C 剪切位点/V659L 1(3.6) c.2168A>G/c.2168A>G H723R /H723R 1(3.6) c.1174A>T/c.1343C>T N392Y/S448X 1(3.6) c.919-2A>G/ 剪切位点 1(3.6) EVAS合并MD c.919-2A>G/c.919-2A>G 剪切位点 14(37.8) c.919-2A>G/c.2168A>G 剪切位点/H723R 4(10.8) c.919-2A>G/589G>A 剪切位点/G197R 2(5.4) c.919-2A>G/c.1229C>T 剪切位点/T410M 2(5.4) c.919-2A>G/c.1174A>T 剪切位点/N392Y 1(2.7) c.919-2A>G/c.414delT 剪切位点/移码 1(2.7) c.919-2A>G/c.1586T>G 剪切位点/I529S 1(2.7) c.919-2A>G/c.1548insC 剪切位点/移码 1(2.7) c.919-2A>G/c.1079C>T 剪切位点/A360V 1(2.7) c.919-2A>G/ivs15+5G>A 剪切位点 1(2.7) c.919-2A>G/c.1825delG 剪切位点/移码 1(2.7) c.919-2A>G/c.1829C>A 剪切位点/S610X 1(2.7) c.919-2A>G/c.1991C>T 剪切位点/A664V 1(2.7) c.919-2A>G/c.2027T>A 剪切位点/L676Q 1(2.7) c.919-2A>G/c.ivs18-1G>A H723R/S532R 1(2.7) c.1174A>T/c.754T>C 剪切位点 1(2.7) c.2168A>G /1594A>C N392Y/S252P 1(2.7) c.2168A>G/1673A>T H723R/N558I 1(2.7) c.1124A>G/c.1409G>A Y375C/R470H 1(2.7) 单独MD c.919-2A>G/ 剪切位点 1(11.1)  下载: 导出CSV
下载: 导出CSV
-
[1] 薛文悦, 陈正侬. SLC26A4基因突变致前庭水管扩大听力损失机制的研究进展[J]. 中华耳科学杂志, 2019, 17(5): 768-772. doi: 10.3969/j.issn.1672-2922.2019.05.029
[2] Koohiyan M. Next generation sequencing and genetics of hereditary hearing loss in the iranian population: New insights from a systematic review[J]. Int J Pediatr Otorhinolaryngol, 2020, 129: 109756. doi: 10.1016/j.ijporl.2019.109756
[3] 袁永一, 戴朴, 朱庆文, 等. 1552例重度感音神经性聋患者与SLC26A4基因IVS7-2 A>G突变相关的全序列分析[J]. 中华耳鼻咽喉头颈外科杂志, 2009, 44(6): 449-454. doi: 10.3760/cma.j.issn.1673-0860.2009.06.003
[4] Mey K, Muhamad AA, Tranebjaerg L, et al. Association of SLC26A4 mutations, morphology, and hearing in pendred syndrome and NSEVA[J]. Laryngoscope, 2019, 129(11): 2574-2579. doi: 10.1002/lary.27319
[5] Huang S, Han D, Yuan Y, et al. Extremely discrepant mutation spectrum of SLC26A4 between Chinese patients with isolated Mondini deformity and enlarged vestibular aqueduct[J]. J Transl Med, 2011, 9: 167. doi: 10.1186/1479-5876-9-167
[6] Dai P, Stewart AK, Chebib F, et al. Distinct and novel SLC26A4/Pendrin mutations in Chinese and U.S. patients with nonsyndromic hearing loss[J]. Physiol Genomics, 2009, 38(3): 281-290. doi: 10.1152/physiolgenomics.00047.2009
[7] Madden C, Halsted M, Meinzen-Derr J, et al. The influence of mutations in the SLC26A4 gene on the temporal bone in a population with enlarged vestibular aqueduct[J]. Arch Otolaryngol Head Neck Surg, 2007, 133(2): 162-168. doi: 10.1001/archotol.133.2.162
[8] Liu Y, Wang L, Feng Y, et al. A New Genetic Diagnostic for Enlarged Vestibular Aqueduct Based on Next-Generation Sequencing[J]. PLoS One, 2016, 11(12): e0168508. doi: 10.1371/journal.pone.0168508
[9] Azaiez H, Yang T, Prasad S, et al. Genotype-phenotype correlations for SLC26A4-related deafness[J]. Hum Genet, 2007, 122(5): 451-457. doi: 10.1007/s00439-007-0415-2
[10] Lee HJ, Jung J, Shin JW, et al. Correlation between genotype and phenotype in patients with bi-allelic SLC26A4 mutations [J]. Clin Genet, 2014, 86(3): 270-275. doi: 10.1111/cge.12273
[11] Tsukamoto K, Suzuki H, Harada D, et al. Distribution and frequencies of PDS(SLC26A4) mutations in Pendred syndrome and nonsyndromic hearing loss associated with enlarged vestibular aqueduct: a unique spectrum of mutations in Japanese[J]. Eur J Hum Genet, 2003, 11(12): 916-922. doi: 10.1038/sj.ejhg.5201073
[12] Choi BY, Stewart AK, Nishimura KK, et al. Efficient molecular genetic diagnosis of enlarged vestibular aqueducts in East Asians[J]. Genet Test Mol Biomarkers, 2009, 13(5): 679-687. doi: 10.1089/gtmb.2009.0054
[13] Lin YH, Wu CC, Lin YH, et al. Targeted Next-Generation Sequencing Facilitates Genetic Diagnosis and Provides Novel Pathogenetic Insights into Deafness with Enlarged Vestibular Aqueduct[J]. J Mol Diagn, 2019, 21(1): 138-148. doi: 10.1016/j.jmoldx.2018.08.007
[14] Lim R, Brichta AM. Anatomical and physiological development of the human inner ear[J]. Hear Res, 2016, 338: 9-21. doi: 10.1016/j.heares.2016.02.004
[15] Pourová R, Janousek P, Jurovcík M, et al. Spectrum and frequency of SLC26A4 mutations among Czech patients with early hearing loss with and without Enlarged Vestibular Aqueduct(EVA)[J]. Ann Hum Genet, 2010, 74(4): 299-307. doi: 10.1111/j.1469-1809.2010.00581.x
[16] Nonose RW, Lezirovitz K, de Mello Auricchio M, et al. Mutation analysis of SLC26A4(Pendrin)gene in a Brazilian sample of hearing-impaired subjects[J]. BMC Med Genet, 2018, 19(1): 73. doi: 10.1186/s12881-018-0585-x
[17] Dai P, Huang LH, Wang GJ, et al. Concurrent Hearing and Genetic Screening of 180, 469 Neonates with Follow-up in Beijing, China[J]. Am J Hum Genet, 2019, 105(4): 803-812. doi: 10.1016/j.ajhg.2019.09.003
[18] 柴福, 赵海亮, 韩晓东, 等. 芯片捕获高通量测序检测耳聋相关基因SLC26A4新突变的意义[J]. 临床耳鼻咽喉头颈外科杂志, 2019, 33(4): 357-361. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH201904018.htm
-
图(3)
表(1)
计量
- 文章访问数: 2581
- PDF下载数: 561
- 施引文献: 0