
The value of quantitative measurement of key structures of inner ear by HRCT in hearing evaluation of patients with congenital severe sensorineural deafness
-
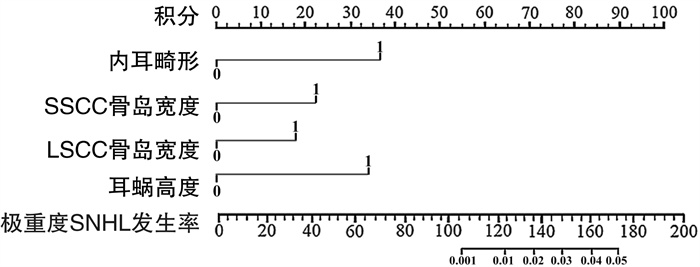
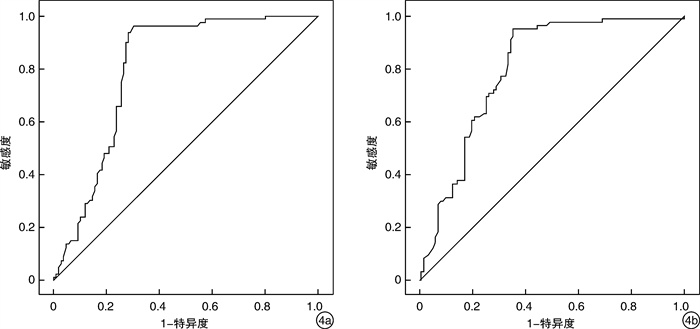
摘要: 目的 探讨内耳关键结构高分辨率CT(HRCT)定量测量在先天性极重度感音神经性聋(SNHL)听力评估中的价值。方法 收集2018年1月—2021年2月于宁波市北仑区人民医院诊治的极重度SNHL患儿90例(180耳)为试验组; 收集同期与试验组年龄相仿, 由于头部外伤怀疑颞骨骨折行颞骨扫描且内耳结构和听力正常的患儿90例(180耳)为对照组。采用Logistic单因素及多因素回归分析影响极重度SNHL发生的因素, 基于多因素分析结果建立Nomogram预测模型, 通过受试者工作特征曲线对内部校正前和校正后的模型进行评价。结果 内耳畸形、SSCC骨岛宽度、LSCC骨岛宽度、耳蜗高度是患儿发生极重度SNHL的独立危险因素; Nomogram预测模型结果显示: 耳蜗高度34分、LSCC骨岛宽度19分、SSCC骨岛宽度22分、内耳畸形37分, 所得总分(112分)对应的值即为极重度SNHL的发生率(0.3%); Nomogram预测模型的实际C-index值为0.858, 内部验证的C-index为0.851, 外部验证的C-index为0.847, 模型的符合度较好。提示该模型能够有效预测先天性SNHL发生的风险因素, 有较高的预测准确度。结论 使用HRCT对SSCC骨岛宽度、LSCC骨岛宽度和耳蜗高度的标准化测量, 对SNHL患儿是否存在微小内耳畸形具有重要的诊断价值。
-
关键词:
- 高分辨率CT /
- 听觉丧失, 感音神经性 /
- 内耳畸形
Abstract: Objective Study on the value of quantitative measurement of key structures of inner ear by high resolution computer tomography(HRCT) in hearing evaluation of patients with congenital severe sensorineural hearing loss(SNHL).Methods A total of 90 children with extremely severe SNHL diagnosed and treated in Beilun District People's Hospital from January 2018 to February 2021 were collected as the experimental group. In the same period, 90 children(180 ears) with normal inner ear structure and hearing were scanned because of head trauma and suspected temporal bone fracture. Logistic univariate and multivariate regression analysis were used to analyze the factors affecting the occurrence of extremely severe SNHL. Based on the results of multivariate analysis, a Nomogram prediction model was established. The model before and after internal correction was evaluated by the receiver working characteristic curve.Results Inner ear malformation, SSCC bone island width, LSCC bone island width and cochlear height were independent risk factors for extremely severe SNHL. The results of Nomogram predictive model showed that cochlear height 34 points, LSCC bone island width 19 points, SSCC bone island width 22 points, inner ear malformation 37 points, the total score(112 points) corresponding to the incidence of extremely severe SNHL(0.3%). The actual C-index value of Nomogram prediction model is 0.858, the C-index of internal verification is 0.851, and the C-index of external verification is 0.847. The coincidence of the model is good. It is suggested that the model can effectively predict the risk factors of congenital extremely severe SNHL and has high prediction accuracy.Conclusion The standardized measurement of SSCC bone island width, LSCC bone island width and cochlear height by HRCT is of great value in the diagnosis of microinner ear malformation in children with extremely severe SNHL. -

-
表 1 测量数据一致性分析mm, x±s
指标 对照组 试验组 A B ICC A B ICC SSCC骨管管腔宽度 0.88±0.05 0.87±0.04 0.812 0.85±0.04 0.88±0.03 0.882 SSCC骨岛宽度 4.43±0.42 4.63±0.47 0.793 4.31±0.41 4.34±0.45 0.841 LSCC骨管管腔宽度 1.50±0.04 1.48±0.03 0.778 1.47±0.05 1.51±0.07 0.799 LSCC骨岛宽度 3.04±0.26 3.05±0.28 0.851 3.01±0.02 3.04±0.04 0.867 PSCC骨管管腔宽度 1.12±0.10 1.07±0.08 0.860 1.08±0.10 1.11±0.12 0.759 PSCC骨脚长度 6.20±0.75 6.18±0.67 0.799 6.14±0.86 6.19±0.88 0.864 耳蜗高度 4.43±0.08 4.45±0.10 0.871 4.49±0.07 4.52±0.09 0.826 耳蜗长度 7.95±0.16 8.02±0.18 0.795 8.00±0.14 8.04±0.14 0.785 前庭宽度 3.19±0.40 3.17±0.38 0.764 3.24±0.38 3.30±0.42 0.844 前庭长度 5.57±0.48 5.62±0.51 0.829 5.64±0.35 5.68±0.43 0.757 耳蜗底周蜗螺旋管径 1.66±0.26 1.68±0.27 0.790 1.64±0.23 1.67±0.25 0.832 内听道口径 5.88±1.27 6.13±1.46 0.836 5.97±1.35 6.09±1.42 0.824 内听道口长径 9.70±1.87 9.55±1.76 0.811 9.68±1.79 9.62±1.74 0.795 内听道口宽径 4.81±0.98 4.85±0.82 0.785 4.84±0.94 4.83±0.97 0.820  下载: 导出CSV
下载: 导出CSV
表 2 2组患儿的单因素方差分析
危险因素 试验组
(n=90)对照组
(n=90)t/F P 危险因素 试验组
(n=90)对照组
(n=90)t/F P 家族史 5.143 0.023 缺氧 4.709 0.030 有 5(5.56) 0(0) 有 7(7.78) 1(1.11) 无 85(94.44) 90(100.00) 无 83(92.22) 89(98.99) 早产 0 1.000 孕期服中药 0 1.000 有 2(2.22) 2(2.22) 有 1(1.11) 1(1.11) 无 88(97.78) 88(97.78) 无 89(98.99) 89(98.99) 难产 0.690 0.406 内耳畸形 8.372 0.004 有 4(4.44) 2(2.22) 有 8(8.89) 0(0) 无 86(95.56) 88(97.78) 无 82(91.11) 90(100.00) SSCC骨管管腔宽度/mm 0.86±0.03 0.85±0.06 1.414 0.159 耳蜗长度/mm 8.01±0.14 8.02±0.16 0.446 0.656 SSCC骨岛宽度/mm 4.21±0.27 4.41±0.30 4.315 < 0.001 前庭宽度/mm 3.26±0.35 3.29±0.39 0.543 0.588 LSCC骨管管腔宽度/mm 1.47±0.17 1.51±0.24 1.780 0.076 前庭长度/mm 5.53±0.21 5.56±0.39 0.643 0.521 LSCC骨岛宽度/mm 3.01±0.01 3.04±0.15 2.538 0.012 耳蜗底周蜗螺旋管径/mm 1.67±0.25 1.69±0.28 0.505 0.614 PSCC骨管管腔宽度/mm 1.08±0.10 1.12±0.51 1.027 0.305 内听道口径/mm 5.80±1.36 6.12±1.42 1.544 0.124 PSCC骨脚长度/mm 6.16±0.82 6.17±0.30 0.158 0.874 内听道口长径/mm 9.53±1.66 9.47±1.72 0.238 0.812 耳蜗高度/mm 4.51±0.07 4.44±0.09 5.824 < 0.001 内听道口宽径/mm 4.78±0.85 4.83±0.86 0.392 0.695
下载: 导出CSV
表 3 极重度SNHL的多因素Logistic回归分析赋值变量表
变量 赋值 极重度SNHL 否=1, 是=0 家族史 有=1, 无=0 围产期缺氧 有=1, 无=0 内耳畸形 有=1, 无=0 SSCC骨岛宽度 ≥4.44 mm=1, <4.44 mm=0 LSCC骨岛宽度 ≥3.04 mm=1, <3.04 mm=0 耳蜗高度 ≥4.49 mm=1, <4.49 mm=0
下载: 导出CSV
表 4 极重度SNHL的多因素Logistic回归分析
影响因素 β SE Wald P OR(95%CI) 家族史 0.542 0.201 7.255 0.138 1.720(0.339~1.943) 围产期缺氧 0.521 0.203 6.591 0.205 1.683(0.422~2.436) 内耳畸形 1.352 0.458 8.703 0.002 3.867(2.225~4.672) SSCC骨岛宽度 0.730 0.241 9.168 0.001 2.076(1.882~2.996) LSCC骨岛宽度 1.245 0.400 9.667 0.001 3.473(3.124~4.882) 耳蜗高度 0.867 0.306 8.044 0.004 2.379(2.003~3.886)
下载: 导出CSV
-
[1] Lee SY, Han JH, Carandang M, et al. Novel genotype-phenotype correlation of functionally characterized LMX1A variants linked to sensorineural hearing loss[J]. Hum Mutat, 2020, 41(11): 1877-1883. doi: 10.1002/humu.24095
[2] Xu XM, Jiao Y, Tang TY, et al. Sensorineural hearing loss and cognitive impairments: Contributions of thalamus using multiparametric MRI[J]. J Magn Reson Imaging, 2019, 50(3): 787-797. doi: 10.1002/jmri.26665
[3] Birkenbeuel J, Abouzari M, Goshtasbi K, et al. Characteristics of Mid-Frequency Sensorineural Hearing Loss Progression[J]. Otol Neurotol, 2019, 40(5): e497-e502. doi: 10.1097/MAO.0000000000002232
[4] Singh R, Rai R, Singh P, et al. High-resolution computed tomography(HRCT)in pediatric and adult patients with unsafe chronic suppurative otitis media(CSOM)and its surgical correlation[J]. J Family Med Prim Care, 2020, 9(8): 4067-4073. doi: 10.4103/jfmpc.jfmpc_455_20
[5] 陈艾婷, 韩莹, 兰兰, 等. 60岁以上门诊老年听力障碍患者听力损失分布的初步研究[J]. 中华耳科学杂志, 2018, 16(4): 445-450. doi: 10.3969/j.issn.1672-2922.2018.04.004
[6] 周霞, 沈桂权, 吴永彦, 等. 先天性重度、极重度感音神经性聋患儿内耳及颅脑影像学评估[J]. 听力学及言语疾病杂志, 2020, 28(1): 83-86. doi: 10.3969/j.issn.1006-7299.2020.01.022
[7] 刘静, 蔡鑫章, 冯永, 等. 经耳内镜慢性化脓性中耳炎手术中上鼓室隔分区比较研究[J]. 中华耳科学杂志, 2019, 17(6): 890-894. doi: 10.3969/j.issn.1672-2922.2019.06.017
[8] Carol Liu YC, Ibekwe T, Kelso JM, et al. Sensorineural hearing loss(SNHL)as an adverse event following immunization(AEFI): Case definition & guidelines for data collection, analysis, and presentation of immunization safety data[J]. Vaccine, 2020, 38(30): 4717-4731. doi: 10.1016/j.vaccine.2020.05.019
[9] Bhandari A, Jain S. Early Intratympanic Methylprednisolone in Sudden SNHL: A Frequency-wise Analysis[J]. Indian J Otolaryngol Head Neck Surg, 2019, 71(3): 390-395. doi: 10.1007/s12070-019-01582-5
[10] 王利利, 宋云韬, 耿曼英, 等. 54例非综合征性前庭导水管扩大的临床分析[J]. 临床耳鼻咽喉头颈外科杂志, 2019, 33(3): 255-258. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH201903018.htm
[11] 赖若沙, 伍伟景, 李葳, 等. 内耳畸形人工耳蜗植入手术难点及其处理[J]. 临床耳鼻咽喉头颈外科杂志, 2020, 34(10): 919-924. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH202010014.htm
[12] Jackler RK, Luxford WM, Brackmann DE, et al. Endolymphatic sac surgery in congenital malformations of the inner ear[J]. Laryngoscope, 1988, 98(7): 698-704.
[13] 刘阳, 赵丹珩, 林勇生. 先天性中耳畸形临床分析及分类探讨[J]. 中华耳鼻咽喉头颈外科杂志, 2019, 54(7): 481-488. doi: 10.3760/cma.j.issn.1673-0860.2019.07.001
[14] de Fraissinette A, Felix H, Hoffmann V, et al. Human Reissner's membrane in patients with age-related normal hearing and with sensorineural hearing loss[J]. ORL J Otorhinolaryngol Relat Spec, 1993, 55(2): 68-72. doi: 10.1159/000276381
[15] 陈彪, 石颖, 拱月, 等. 耳蜗不全分隔畸形患儿耳蜗形态与人工耳蜗术后效果评估[J]. 中华耳科学杂志, 2020, 18(6): 1066-1071. doi: 10.3969/j.issn.1672-2922.2020.06.013
-
图(4)
表(4)
计量
- 文章访问数: 1497
- PDF下载数: 484
- 施引文献: 0