
Experience in the diagnosis and treatment of the postoperative complications of craniopharyngiomas through expanded endoscopic endonasal transsphenoidal approach
-
摘要: 目的 总结内镜下扩大经鼻蝶入路治疗颅咽管瘤术后并发症的特点及治疗措施。方法 回顾性分析15例行内镜扩大经鼻蝶手术切除颅咽管瘤患者的临床资料, 记录术后并发症的发生情况。结果 15例颅咽管瘤患者中, 肿瘤部分切除11例, 近全切除4例。术后主要并发症: 腺垂体功能减退(11/15), 尿崩症(8/15), 鼻出血(3/15), 脑脊液鼻漏(1/15)。给予对症或再次手术治疗, 好转10例, 嗜睡1例, 多器官衰竭3例, 死亡1例。结论 内镜下扩大经鼻蝶入路治疗颅咽管瘤手术术前需充分评估、掌握好手术适应证, 术中保护重要的神经血管, 避免损伤正常垂体、下丘脑, 完善颅底重建, 以预防和减少术后并发症的发生。鼻内镜的标准步骤以及临床医师的手术经验非常重要, 且需多学科共同合作。Abstract: Objective To summarize the clinical characteristics of the postoperative complications of surgical resection of craniopharyngiomas through expanded endoscopic endonasal transsphenoidal approach (EEETA). Strategies for prevention and management were also discussed.Methods The clinical data of the patients who were treated through EEETA were retrospectively reviewed. The occurrence of post-operative complications were recorded.Results Partial removal of the tumors were accomplished in 11 cases and subtotal removal in 4 cases. The major postoperative complications were anterior pituitary hypofunction(11/15), diabetes insipidus(8/15), epistaxis(3/15), cerebrospinal fluid rhinorrhea(1/15). The cases were treated symptomatically or by re-operation. Of all the cases, 10 patients were improved, 1 patient had drowsiness, 3 suffered from multiple organ failure, and 1 patient died.Conclusion To prevent and reduce the postoperative complications of EEETA, first of all, it is essential to evaluate the need for surgical intervention and perform a comprehensive preoperative assessment. Critical nerves and vessels should be preserved carefully during operation for the sake of avoiding injuries normal pituitary and hypothalamus. Furthermore, reconstruction of the skull base is critical. The standard procedure of nasal endoscopy and the experience of the surgeons are quite significant, while the operation needs multidisciplinary collaborations.
-
Key words:
- endoscopy /
- endonasal transsphenoidal approach /
- craniopharyngioma /
- complications
-

-
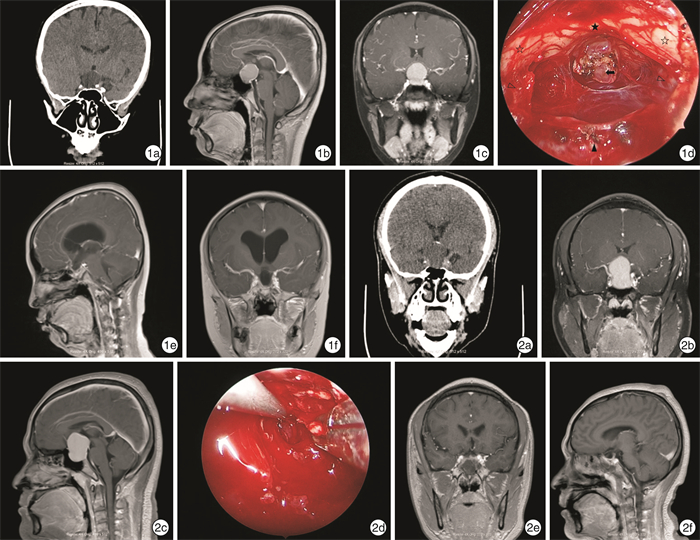
图 1 病例8资料 1a:术前头部CT;1b、1c:术前头部MRI增强;1d:术中所见肿物,☆示视神经,★示视交叉,△示颈内动脉,▲示垂体窝,↑示垂体柄残端病变起源处;1e、1f:术后半年复查头部MRI增强;图 2 病例15资料 2a:术前头部CT;2b、2c:术前头部MRI增强;2d:术中所见肿物;2e、2f:术后7 d头部MRI增强。
表 1 15例颅咽管瘤患者临床资料
例序 性别 年龄/岁 位置 肿瘤切除程度 鞍区周围受侵情况 术后主要并发症 出院时情况 1 女 58 鞍区+鞍上 部分切除 三脑室及侧脑室扩张,双侧海绵窦受压,鞍底骨质受压下陷 尿崩症、垂体功能减退、脑脊液鼻漏、颅内感染、鼻出血、感染性休克、贫血 好转 2 女 23 鞍区 近全切除 双侧海绵窦轻度受压 呼吸性碱中毒 好转 3 男 76 鞍区 部分切除 双侧颈内动脉海绵窦段受压 垂体功能减退、吸入性肺炎、房颤、肺感染、颅内感染、低蛋白血症 多器官衰竭 4 女 61 鞍区+鞍上 部分切除 向上突入鞍上池,鞍底骨质受压下陷 尿崩症、垂体功能减退、鼻出血 好转 5 女 51 鞍区+鞍上 部分切除 向上部分突入鞍上池,双侧海绵窦受压,鞍底骨质受压下陷 尿崩症、垂体功能减退 好转 6 女 66 鞍区+鞍上 部分切除 向上部分突入鞍上池,鞍底骨质受压下陷 尿崩症、垂体功能减退、颅内感染、贫血、低蛋白血症 多器官衰竭 7 男 67 鞍区 部分切除 双侧海绵窦受压 垂体功能减退、鼻出血 好转 8 男 13 鞍区+鞍上 部分切除 向上部分突入鞍上池,三脑室受压 尿崩症、垂体功能减退、颅内感染 好转 9 男 67 鞍区+鞍上 部分切除 向上部分突入鞍上池 垂体功能减退、呼吸衰竭、肺感染 死亡 10 女 63 鞍区+鞍上 部分切除 向上部分突入鞍上池,双侧海绵窦受压 尿崩症、垂体功能减退、肺部感染、贫血 嗜睡 11 男 56 鞍区+鞍上 近全切除 向上部分突入鞍上池,鞍底骨质受压下陷 垂体功能减退、脑室出血、颅内感染 多器官衰竭 12 男 71 鞍区+鞍上 部分切除 向上部分突入鞍上池 尿崩症、垂体功能减退、颅内感染、低蛋白血症 好转 13 男 51 鞍区 部分切除 鞍底骨质变薄 尿崩症、垂体功能减退 好转 14 男 63 鞍内、左鞍旁、蝶窦、左侧筛窦及左侧眶内 近全切除 左侧海绵窦受压,相邻鞍底、蝶窦及左侧筛窦壁骨质破坏 垂体功能减退 好转 15 男 34 鞍区+鞍上 近全切除 向上突入鞍上池,三脑室受压,双侧海绵窦受压 垂体功能减退 好转  下载: 导出CSV
下载: 导出CSV
-
[1] Müller HL, Merchant TE, Warmuth-Metz M, et al. Craniopharyngioma[J]. Nat Rev Dis Primers, 2019, 5(1): 75. doi: 10.1038/s41572-019-0125-9
[2] Sankhla SK, Jayashankar N, Khan GM. Extended endoscopic endonasal transsphenoidal approach for retrochiasmatic craniopharyngioma: Surgical technique and results[J]. J Pediatr Neurosci, 2015, 10(4): 308-316. doi: 10.4103/1817-1745.174457
[3] Komotar RJ, Roguski M, Bruce JN. Surgical management of craniopharyngiomas[J]. J Neurooncol, 2009, 92(3): 283-296. doi: 10.1007/s11060-009-9841-4
[4] Locatelli D, Levi D, Rampa F, et al. Endoscopic approach for the treatment of relapses in cystic craniopharyngiomas[J]. Childs Nerv Syst, 2004, 20(11/12): 863-867.
[5] Fernandez-Miranda JC, Gardner PA, Snyderman CH, et al. Craniopharyngioma: a pathologic, clinical, and surgical review[J]. Head Neck, 2012, 34(7): 1036-1044. doi: 10.1002/hed.21771
[6] Jane JA Jr, Prevedello DM, Alden TD, et al. The transsphenoidal resection of pediatric craniopharyngiomas: a case series[J]. J Neurosurg Pediatr, 2010, 5(1): 49-60.
[7] Komotar RJ, Starke RM, Raper DM, et al. Endoscopic endonasal compared with microscopic transsphenoidal and open transcranial resection of craniopharyngiomas[J]. World Neurosurg, 2012, 77(2): 329-341. doi: 10.1016/j.wneu.2011.07.011
[8] Elliott RE, Jane JA Jr, Wisoff JH. Surgical management of craniopharyngiomas in children: meta-analysis and comparison of transcranial and transsphenoidal approaches[J]. Neurosurgery, 2011, 69(3): 630-643. doi: 10.1227/NEU.0b013e31821a872d
[9] Koutourousiou M, Gardner PA, Fernandez-Miranda JC, et al. Endoscopic endonasal surgery for craniopharyngiomas: surgical outcome in 64 patients[J]. J Neurosurg, 2013, 119(5): 1194-1207. doi: 10.3171/2013.6.JNS122259
[10] 颅咽管瘤治疗专家共识编写委员会, 中华医学会神经外科学分会小儿神经外科学组. 颅咽管瘤患者长期内分泌治疗专家共识(2017)[J]. 中华医学杂志, 2018, 98(1): 11-18. doi: 10.3760/cma.j.issn.0376-2491.2018.01.004
[11] Campbell PG, McGettigan B, Luginbuhl A, et al. Endocrinological and ophthalmological consequences of an initial endonasal endoscopic approach for resection of craniopharyngiomas[J]. Neurosurg Focus, 2010, 28(4): E8. doi: 10.3171/2010.1.FOCUS09292
[12] Cavallo LM, Frank G, Cappabianca P, et al. The endoscopic endonasal approach for the management of craniopharyngiomas: a series of 103 patients[J]. J Neurosurg, 2014, 121(1): 100-113. doi: 10.3171/2014.3.JNS131521
[13] Frank G, Pasquini E, Doglietto F, et al. The endoscopic extended transsphenoidal approach for craniopharyngiomas[J]. Neurosurgery, 2006, 59(1 Suppl 1): ONS75-83.
[14] 张胜男, 姜彦, 于龙刚, 等. 鼻内镜下脑脊液鼻漏修补术诊疗分析[J]. 临床耳鼻咽喉头颈外科杂志, 2019, 33(12): 1189-1195, 1199. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH201912019.htm
[15] Hadad G, Bassagasteguy L, Carrau RL, et al. A novel reconstructive technique after endoscopic expanded endonasal approaches: vascular pedicle nasoseptal flap[J]. Laryngoscope, 2006, 116(10): 1882-1886. doi: 10.1097/01.mlg.0000234933.37779.e4
[16] 翟翔, 张金玲, 王茹媛, 等. 内镜术后鼻腔严重继发性出血的处理策略[J]. 中华医学杂志, 2019, 99(10): 783-786.
-
图(1)
表(1)
计量
- 文章访问数: 1626
- PDF下载数: 496
- 施引文献: 0