
Pathologic tumor volume predicting survival outcomes of patients with local advanced glottic carcinoma
-
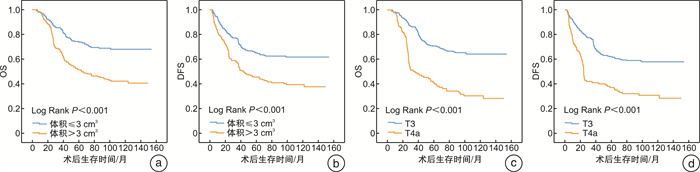
摘要: 目的 分析局部晚期声门型喉癌术后在病理学上测量的肿瘤体积和患者的总生存率(OS)和无病生存率(DFS)的关系。 方法 收集2005年1月-2010年12月接受手术±放/化疗的406例T3~T4期声门型喉鳞状细胞癌患者的病理和临床数据并进行随访。统计患者的临床信息,计算术后病理肿瘤体积,ROC曲线获取二分类最佳界值。Logistic回归模型分析患者的肿瘤体积与T分期的关系,Cox回归模型分析肿瘤体积与OS和DFS的关系。 结果 406例声门型喉癌患者5年和10年的OS分别为62.9%和55.4%,DFS分别为55.5%和50.8%。肿瘤体积为(5.1±6.7) cm3,T4期患者的肿瘤体积较T3期大(P < 0.001)。Logistic回归模型发现肿瘤体积和T分期具有相关性,影响T分期(OR=13.81,95%CI:6.03~31.59,P < 0.001)。ROC曲线获得OS和DFS的肿瘤体积的最佳界值为3 cm3,肿瘤体积≤3 cm3患者的OS和DFS高于肿瘤体积>3 cm3的患者(P < 0.001)。采用Cox回归模型排除混杂因素,发现肿瘤体积是影响患者OS和DFS的独立危险因素(OS:HR=1.59,95%CI:1.09~2.32,P=0.017;DFS:HR=1.54,95%CI:1.08~2.20,P=0.016)。 结论 肿瘤体积和T分期具有相关性,是影响局部晚期声门型喉癌患者生存率的独立危险因素。Abstract: Objective The aim of this study was to evaluate the predicting role of tumor volume as evaluated by postoperative pathologic examination on overall survival(OS) and disease free survival(DFS) in patients with local advanced glottic carcinoma. Methods In this study, the records of 406 consecutive patients with local advanced glottic carcinoma(T3-T4 stages) who underwent surgery ± chemoradiotherapy from January 2005 to December 2010 were retrospectively reviewed and followed up. The demographic characteristics, disease staging, and pathologic tumor volume were analyzed. The optimal cutoff values of tumor volume for OS and DFS were obtained by using receiver operating characteristic(ROC) curves. The association of tumor volume with T stages were assessed by using Logistic regression model, and the relationship between tumor volume and OS and DFS rates were evaluated by using Cox regression models. Results The 5-and 10-year OS rates were 62.9% and 55.4%, respectively. The 5-and 10-year DFS rates were 55.5% and 50.8%, respectively. The mean tumor volume was(5.1±6.7) cm3, T4 stage patients had higher tumor volume than those of patients with T3 stage(P < 0.001). The factor of tumor volume was correlated with T stages by using Logistic regression analyses(OR = 13.81, 95%CI: 6.03-31.59, P < 0.001). The optimal cutoff values of tumor volume that were both at 3 cm3 for OS and DFS rates were obtained by using ROC curve plots. The OS and DFS rates of glottic carcinoma patients with tumor volume ≤ 3 cm3 were better when compared with those of patients with tumor volume>3 cm3(P < 0.001). Upon multivariate analyses, tumor volume was strongly correlated with poorer OS and DFS rates and remained independent prognostic factors for both the OS and DFS of patients with glottic carcinoma(OS: HR = 1.59, 95%CI: 1.09-2.32, P=0.017; DFS: HR = 1.54, 95%CI: 1.08-2.20, P = 0.016). Conclusion This study demonstrates that tumor volume is correlated with T stages, and this factor is an independent predictive factor of survival outcomes in patients with local advanced glottic carcinoma.
-
Key words:
- laryngeal neoplasms /
- tumor volume /
- survival rate
-

-
表 1 406例局部晚期声门型喉癌患者的临床资料
肿瘤体积≤3 cm3 (n=206) 肿瘤体积>3 cm3 (n=200) P 肿瘤体积≤3 cm3 (n=206) 肿瘤体积>3 cm3 (n=200) P 年龄/岁 0.002a) N分期 < 0.001b) 平均值 59.3±10.5 62.5±10.4 N0 198(96.1) 155(77.5) 范围 30~83 36~85 N1 3(1.5) 19(9.5) 年龄分组/岁 < 0.001b) N2 5(2.4) 22(11.0) ≤50 44(21.4) 28(14.0) N3 0(0.0) 4(2.0) 51~60 75(36.4) 60(30.0) 临床分期 < 0.001c) 61~70 53(25.7) 56(28.0) Ⅲ 192(93.2) 93(46.5) >70 34(16.5) 56(28.0) Ⅳ 14(6.8) 107(53.5) 性别 0.022c) 手术方式 < 0.001c) 男性 196(95.1) 198(99.0) 喉部分切除术 98(47.6) 8(4.0) 女性 10(4.9) 2(1.0) 全喉切除术 108(52.4) 192(96.0) 吸烟史 0.568c) 病理分级 0.488d) 吸烟 143(69.4) 144(72.0) 中高分化 198(96.1) 193(96.5) 不吸烟 63(30.6) 56(28.0) 低分化 4(1.9) 5(2.5) 饮酒史 0.482c) 未知 4(1.9) 2(1.0) 饮酒 102(49.5) 106(53.0) 既往史 0.122c) 不饮酒 104(50.5) 94(47.0) 有高血压和/或糖尿病 50(24.3) 36(18.0) T分期 < 0.001c) 无高血压和/或糖尿病 156(75.7) 164(82.0) T3 197(95.6) 104(52.0) T4 9(4.4) 96(48.0) 注:a)采用t检验;b)采用秩和检验;c)采用卡方检验;d)采用Fish检验。  下载: 导出CSV
下载: 导出CSV
表 2 406例局部晚期声门型喉癌患者3、5、10年的OS和DFS比较
% 3年 5年 10年 P OS DFS OS DFS OS DFS 肿瘤体积/ cm3 76.2 66.9 62.9 55.5 55.4 50.8 < 0.001 ≤3 85.4 76.7 73.7 65.1 68.0 61.6 >3 66.7 56.9 51.7 45.6 42.3 39.4 T分期 < 0.001 T3 85.6 76.0 70.9 62.0 64.2 57.8 T4 49.2 40.8 40.3 37.0 30.6 30.9
下载: 导出CSV
表 3 肿瘤体积和T分期的Logistic相关性分析
变量 T3患者 T4患者 单因素分析 多因素分析 OR 95%CI P HR 95%CI 校正后Pa) 肿瘤体积/cm3 ≤3 197 9 >3 104 96 20.21 9.80~41.65 < 0.001 13.81 6.03~31.59 < 0.001 注:a)多因素回归模型分析的变量包括性别、年龄、吸烟、饮酒、N分期、病理分期、既往病史、术后放化疗、手术方式和肿瘤体积。
下载: 导出CSV
表 4 单因素和多因素Cox回归模型分析影响局部晚期声门型喉癌OS和DFS的因素
变量 单因素分析 多因素分析 HR 95%CI P HR 95%CI 校正后P OS 肿瘤体积/cm3 ≤3 1 1 >3 2.22 1.63~3.02 < 0.001 1.59 1.09~2.32 0.017a) T分期 T3 1 1 T4 2.88 2.12~3.90 < 0.001 2.32 1.66~3.26 < 0.001b) DFS 肿瘤体积/cm3 ≤3 1 1 >3 1.95 1.46~2.60 < 0.001 1.54 1.08~2.20 0.016a) T分期 T3 1 1 T4 2.35 1.76~3.15 < 0.001 2.12 1.53~2.94 < 0.001b) 注:a)多因素回归模型分析的变量包括性别、年龄、吸烟、饮酒、T分期、N分期、病理分期、术后放化疗、手术方式、既往病史和肿瘤体积;b)多因素回归模型分析的变量包括性别、年龄、吸烟、饮酒、T分期、N分期、病理分期、术后放化疗、手术方式、既往病史。
下载: 导出CSV
-
[1] Liu Y, Zhao Q, Ding G, et al. Incidence and mortality of laryngeal cancer in China, 2008-2012[J]. Chin J Cancer Res, 2018, 30(3): 299-306. doi: 10.21147/j.issn.1000-9604.2018.03.02
[2] 李梦婷, 夏立军, 李锦荣. 晚期喉癌的治疗进展[J]. 中国耳鼻咽喉颅底外科杂志, 2020, 26(3): 343-348. https://www.cnki.com.cn/Article/CJFDTOTAL-ZEBY202003028.htm
[3] 乐慧君, 陈思宇, 李芸, 等. 喉癌诊疗策略及进展[J]. 临床耳鼻咽喉头颈外科杂志, 2019, 33(11): 1017-1021. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH201911003.htm
[4] Tomayko MM, Reynolds CP. Determination of subcutaneous tumor size in athymic(nude)mice[J]. Cancer Chemother Pharmacol, 1989, 24(3): 148-154. doi: 10.1007/BF00300234
[5] 雷大鹏, 潘新良. 中晚期喉癌的治疗选择[J]. 中华耳鼻咽喉头颈外科杂志, 2019, 54(5): 398-400. doi: 10.3760/cma.j.issn.1673-0860.2019.05.018
[6] 王军, 崔晓波, 孙源昊. 诱导化疗在局晚期喉癌下咽癌治疗中的意义[J]. 临床耳鼻咽喉头颈外科杂志, 2016, 30(19): 1548-1551. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH201619012.htm
[7] Timmermans AJ, van Dijk BA, Overbeek LI, et al. Trends in treatment and survival for advanced laryngeal cancer: A 20-year population-based study in The Netherlands[J]. Head Neck, 2016, 38 Suppl 1: E1247-E1255.
[8] Megwalu UC, Sikora AG. Survival outcomes in advanced laryngeal cancer[J]. JAMA Otolaryngol Head Neck Surg, 2014, 140(9): 855-860. doi: 10.1001/jamaoto.2014.1671
[9] Studer G, Lütolf UM, El-Bassiouni M, et al. Volumetric staging(VS)is superior to TNM and AJCC staging in predicting outcome of head and neck cancer treated with IMRT[J]. Acta Oncol, 2007, 46(3): 386-394. doi: 10.1080/02841860600815407
[10] Dziegielewski PT, Reschly WJ, Morris CG, et al. Tumor volume as a predictor of survival in T3 glottic carcinoma: A novel approach to patient selection[J]. Oral Oncol, 2018, 79: 47-54. doi: 10.1016/j.oraloncology.2018.02.015
[11] Hsin LJ, Fang TJ, Tsang NM, et al. Tumor volumetry as a prognostic factor in the management of T4a laryngeal cancer[J]. Laryngoscope, 2014, 124(5): 1134-1140. doi: 10.1002/lary.24461
[12] Shiao JC, Mohamed A, Messer JA, et al. Quantitative pretreatment CT volumetry: Association with oncologic outcomes in patients with T4a squamous carcinoma of the larynx[J]. Head Neck, 2017, 39(8): 1609-1620. doi: 10.1002/hed.24804
[13] Hoebers F, Rios E, Troost E, et al. Definitive radiation therapy for treatment of laryngeal carcinoma: impact of local relapse on outcome and implications for treatment strategies[J]. Strahlenther Onkol, 2013, 189(10): 834-841. doi: 10.1007/s00066-013-0414-2
[14] 瞿姣, 张梦梅, 韦文彦, 等. 喉癌术前T分期的CT及MRI研究现状与进展[J]. 临床耳鼻咽喉头颈外科杂志, 2020, 34(5): 470-474. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH202005023.htm
[15] Gallo O, Sarno A, Baroncelli R, et al. Multivariate analysis of prognostic factors in T3 N0 laryngeal carcinoma treated with total laryngectomy[J]. Otolaryngol Head Neck Surg, 2003, 128(5): 654-662. doi: 10.1016/S0194-5998(03)00228-6
[16] Eskiizmir G, Tanyeri Toker G, Celik O, et al. Predictive and prognostic factors for patients with locoregionally advanced laryngeal carcinoma treated with surgical multimodality protocol[J]. Eur Arch Otorhinolaryngol, 2017, 274(3): 1701-1711. doi: 10.1007/s00405-016-4411-9
[17] 宋晓霞, 皇甫辉, 李莉. 影响喉癌患者预后的多因素分析[J]. 中国耳鼻咽喉颅底外科杂志, 2020, 26(3): 306-311. https://www.cnki.com.cn/Article/CJFDTOTAL-ZEBY202003018.htm
-
图(1)
表(4)
计量
- 文章访问数: 988
- PDF下载数: 312
- 施引文献: 0