
-
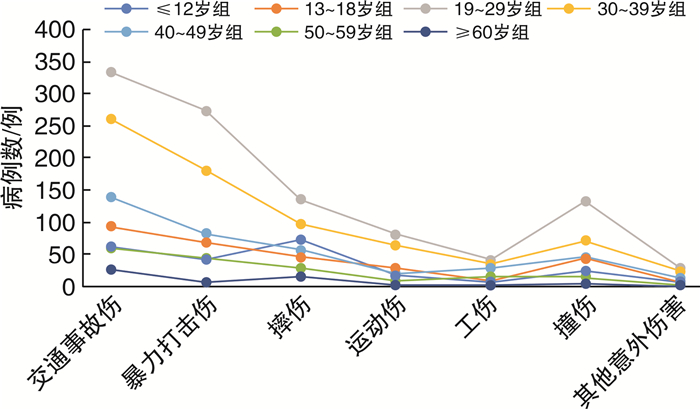
摘要: 目的 对鼻骨骨折患者进行相关的临床流行病学概括和分析。方法 回顾性总结2 881例鼻骨骨折住院患者的临床资料,并对其性别、年龄、骨折类型、致伤原因等情况进行综合分析。采用Fred分型方法对鼻骨骨折进行分型,采用SPSS 25.0软件完成统计分析。结果 鼻骨骨折男女比例为2.44:1,总体男性患者多于女性。19~29岁组鼻骨骨折患者最多(35.54%)。交通事故伤发生率最高(33.84%),其次是暴力打击伤(24.12%)。统计分析表明,鼻骨合并上颌骨额突骨折患者多于单纯性鼻骨骨折患者,Ⅱ型鼻骨骨折患者明显多于其他骨折类型患者。对单纯性鼻骨骨折进行Logistic回归分析发现,男性发生单纯性鼻骨骨折的相对危险度较低。且随着患者年龄的增长,发生单纯性鼻骨骨折的风险降低。相对于车祸伤而言,病因为暴力伤、运动伤、撞伤时,发生单纯性鼻骨骨折的相对危险度较高。结论 鼻骨骨折住院患者在个体特征、创伤原因、部位等方面具有一定的分布规律,应深入展开相关防治性的策略研究。Abstract: Objective This thesis studies on epidemiological characteristics of patients with nasal bone fractures.Method This thesis retrospectively studies on 2 881 patients with nasal bone fractures. The characteristics, causes, and fracture types are collected and reviewed retrospectively. The type of nasal bone fracture is classified according to Fred's classification, and SPSS 25.0 software is used in statistical analysis.Result The sex ratio of nasal bone fracture between males and females is 2.44 : 1, male cases are obviously more than female cases. The group aged 19-29 years occupies the largest proportion, accounted for 35.54%. Traffic accident was the leading cause of the nasal bone fracture, accounting for 33.84%. The second cause was violent assault, 24.12% totally. The number of patients suffering nasal bone fractures combined with maxilla frontal process fractures is higher than that of simple nasal bone fractures. Type Ⅱ fracture is significantly more common in patients with other types nasal bone fractures. Logistic regression analysis for simple nasal bone fracture showed that the relative risk of simple nasal bone fracture is lower in men than in women, and the risk of simple nasal fractures decreased with age increasing. Compared with traffic accident, the relative risk of simple nasal bone fracture is higher in violence injury, sports injury and collision injury.Conclusion The distribution of the nasal fractures of the inpatients has certain characteristics in terms of individual characteristics, injury cause and fracture types, which is worthy of further strategic study on prevention and treatment of the nasal fractures.
-
Key words:
- nasal bone fracture /
- epidemiology /
- retrospective study
-

-
表 1 年龄分组
组别 性别 合计 构成比/% 男 女 ≤12岁组 152 75 227 7.88 13~18岁组 241 52 293 10.17 19~29岁组 729 295 1024 35.54 30~39岁组 493 237 730 25.34 40~49岁组 254 129 383 13.29 50~59岁组 132 38 170 5.90 ≥60岁组 42 12 54 1.87 合计 2 043 838 2 881 100.00  下载: 导出CSV
下载: 导出CSV
表 2 鼻骨骨折及合并周围骨折情况
例(%) 侧别 单纯性鼻骨骨折 合并上颌骨额突骨折 鼻眶筛骨折 合并颌面部其他骨折 合计 左侧 186(6.46) 172(5.97) 42(1.46) 6(0.21) 406(14.09) 右侧 178(6.18) 153(5.31) 17(0.59) 5(0.17) 353(12.25) 双侧 663(23.01) 1120(38.88) 282(9.79) 57(1.98) 2122(73.65) 合计 1027(35.65) 1445(50.16) 341(11.84) 68(2.36) 2881(100.00)
下载: 导出CSV
表 3 单纯性鼻骨骨折多因素风险分析
因素 单纯性鼻骨骨折 调整前P值 OR值 95%CI 调整后P值 是(n=1 027) 否(n=1 854) 性别 男 701(68.26) 1342(72.38) 0.020 0.807 0.681~0.955 0.013 女 326(31.74) 512(27.62) — — — — 年龄/岁 27.54±11.83 31.03±13.65 < 0.001 0.978 0.972~0.985 < 0.001 病因 车祸伤 320(31.2) 655(35.3) — 1.000 — — 暴力伤 264(25.7) 431(23.2) 0.029 1.244 1.103~1.527 0.037 摔伤 148(14.4) 300(16.2) 0.936 0.949 0.746~1.208 0.671 运动伤 92(9.0) 127(6.9) 0.010 1.410 1.042~1.909 0.026 工伤 33(3.2) 100(5.4) 0.064 0.715 0.470~1.087 0.117 撞伤 142(13.8) 190(10.2) 0.001 1.453 1.123~1.881 0.005 其他 28(2.7) 51(2.8) 0.634 1.078 0.664~1.749 0.762
下载: 导出CSV
-
[1] James JG, Izam AS, Nabil S, et al. Closed and Open Reduction of Nasal Fractures[J]. J Craniofac Surg, 2020, 31(1): e22-e26. doi: 10.1097/SCS.0000000000005812
[2] Yu H, Jeon M, Kim Y, et al. Epidemiology of violence in pediatric and adolescent nasal fracture compared with adult nasal fracture: An 8 years study[J]. Arch Craniofac Surg, 2019, 20(4): 228-232. doi: 10.7181/acfs.2019.00346
[3] Das TA, AslamAS, Mangalath U, et al. Evaluation of Treatment outcome Following Closed Reduction of Nasal bone fractures[J]. J Contemp Dent Pract, 2018, 19(10): 1174-1180. doi: 10.5005/jp-journals-10024-2402
[4] Kim KS, Lee HG, Shin JH, et al. Trend analysis of nasal bone fracture[J]. Arch Craniofac Surg, 2018, 19(4): 270-274. doi: 10.7181/acfs.2018.02264
[5] Arnold MA, Yanik SC, Suryadevara AC. Septal fractures predict poor outcomes after closed nasal reduction: Retrospective review and survey[J]. Laryngoscope, 2019, 129(8): 1784-1790. doi: 10.1002/lary.27781
[6] Lee JJ, Hong SD, Dhong HJ, et al. Risk factors for intraoperative saddle nose deformity in septoplasty patients[J]. Eur Arch Otorhinolaryngol, 2019, 276(7): 1981-1986. doi: 10.1007/s00405-019-05411-x
[7] Basheeth N, Donnelly M, David S, et al. Acute nasal fracture management: A prospective study and literature review[J]. Laryngoscope, 2015, 125(12): 2677-2684. doi: 10.1002/lary.25358
[8] Byun IH, Lee WJ, Roh TS, et al. Demographic Factors of Nasal Bone Fractures and Social Reflection[J]. J Craniofac Surg, 2020, 31(1): 169-171. doi: 10.1097/SCS.0000000000006065
[9] Yu H, Jeon M, Kim Y, et al. Epidemiology of violence in pediatric and adolescent nasal fracture compared with adult nasal fracture: An 8-year study[J]. Arch Craniofac Surg, 2019, 20(4): 228-232. doi: 10.7181/acfs.2019.00346
[10] Fred GF, Michael PO, Todd WP, et al. Management of nasal trauma to the nasal bones and septum[M]//Fred JS, Chris DS, Guy SK, eds. Rhinology and Facial Plastic Surgery. Germany: Springer-Verlag Berlin Heidelberg, 2009: 793-799.
[11] Kuhr E, Werner JA, Dietz A, et al. Analysis of the emergency patients of a university ENT hospital[J]. Laryngorhinootologie, 2019, 98(9): 625-630. doi: 10.1055/a-0916-8916
[12] Li K, Moubayed SP, Spataro E, et al. Risk Factors for Corrective Septorhinoplasty Associated With Initial Treatment of Isolated Nasal Fracture[J]. JAMA Facial Plast Surg, 2018, 20(6): 460-467. doi: 10.1001/jamafacial.2018.0336
[13] Hwang K, You SH, Kim SG, et al. Analysis of nasal bone fractures: a six-year study of 503 patients[J]. J Craniofac Surg, 2006, 17(2): 261-264. doi: 10.1097/00001665-200603000-00010
[14] Pham TT, Lester E, Grigorian A, et al. National Analysis of Risk Factors for Nasal Fractures and Associated Injuries in Trauma[J]. Craniomaxillofac Trauma Reconstr, 2019, 12(3): 221-227. doi: 10.1055/s-0039-1677724
[15] Lee KH, Qiu M. Characteristics of Alcohol-Related Facial Fractures[J]. J Oral Maxillofac Surg, 2017, 75(4): 786. e1-786. e7. doi: 10.1016/j.joms.2016.12.018
[16] Emodi O, Wolff A, Srouji H, et al. Trend and Demographic Characteristics of Maxillofacial Fractures in Level I Trauma Center[J]. J Craniofac Surg, 2018, 29(2): 471-475. doi: 10.1097/SCS.0000000000004128
[17] Kang BH, Kang HS, Han JJ, et al. A retrospective clinical investigation for the effectiveness of closed reduction on nasal bone fracture[J]. Maxillofac Plast Reconstr Surg, 2019, 41(1): 53. doi: 10.1186/s40902-019-0236-y
[18] Menon S, Sham ME, Kumar V, et al. Maxillofacial Fracture Patterns in Road Traffic Accidents[J]. Ann Maxillofac Surg, 2019, 9(2): 345-348. doi: 10.4103/ams.ams_136_19
[19] Han DS, Han YS, Park JH, et al. A new approach to the treatment of nasal bone fracture: radiologic classification of nasal bone fractures and its clinical application[J]. J Oral Maxillofac Surg, 2011, 69(11): 2841-2847. doi: 10.1016/j.joms.2011.01.013
[20] Murray JA, Maran AG, Busuttil A, et al. A pathological classification of nasal fractures[J]. Injury, 1986, 17(5): 338-344. doi: 10.1016/0020-1383(86)90159-2
[21] Boffano P, Roccia F, Zavattero E, et al. European Maxillofacial Trauma(EURMAT)in children: a multicenter and prospective study[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2015, 119(5): 499-504. doi: 10.1016/j.oooo.2014.12.012
[22] Pham TT, Lester E, Grigorian A, et al. National Analysis of Risk Factors for Nasal Fractures and Associated Injuries in Trauma[J]. Craniomaxillofac Trauma Reconstr, 2019, 12(3): 221-227. doi: 10.1055/s-0039-1677724
-

图(2)
表(3)
计量
- 文章访问数: 941
- PDF下载数: 532
- 施引文献: 0