
Diagnosis and outcome analysis of diseases characterized by recurrent low-frequency sensorineural deafness
-
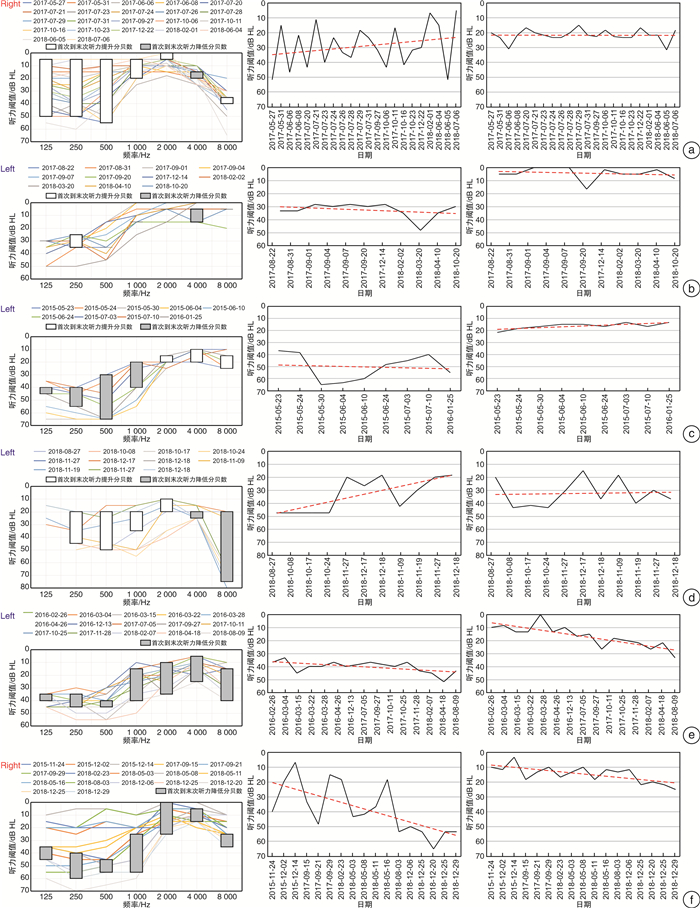
摘要: 目的 初步探索波动性低频感音神经性聋(RLFD)的临床特征、听力学预后和相关疾病的鉴别。认识以RLFD为特征的疾病发展及变化规律。方法 回顾性分析RLFD患者的病史特征、临床表现、听力学检查、辅助检查等资料,总结临床特征,绘制纯音测听变化曲线,明确部分以RLFD为临床表现的疾病的诊断,分析其听力学转归。结果 47例(53耳)RLFD患者听力复查时间为1~124个月,中位数为8个月;病程3~320个月,平均29个月。①伴随症状中耳鸣44例(93.6%),耳闷39例(83.0%),18例(38.3%)患者在病程发展过程中出现了前庭症状;②明确诊断相关疾病27例(57.4%),其中7例(14.9%)梅尼埃病,6例(12.8%)前庭性偏头痛,2例(4.3%)梅尼埃病与偏头痛共病,1例(2.1%)为特发性颅内低血压,11例(23.4%)为可能的耳蜗性偏头痛;③偏头痛相关的RLFD发病年龄更小,女性多见;④在观察期间,44耳(83.0%)低频听力稳定或有所提高,9耳(17.0%)低频听阈的听力损失加重;⑤10耳(18.9%)高频听力下降;⑥RLFD有6种听力学转归类型:低频改善合并高频稳定型;低频稳定合并高频稳定型;低频进展合并高频稳定型;低频改善合并高频进展型;低频稳定合并高频进展型;低频进展合并高频进展型;⑦上升型听力曲线低频听力预后较好,山型和下降型低频听力预后较差。结论 耳鸣、耳闷是较早出现且最困扰RLFD患者的症状,偏头痛相关机制可能在RLFD的发病中起到重要的作用,且女性多见,发病年龄小。低颅压综合征等罕见病因亦不容忽视。RLFD长期波动后听力大多稳定或有提升,但部分患者低频和高频听力都可能下降,初始听力曲线类型是预后的影响因素,长期听力随访有助于评估预后。
-
关键词:
- 听觉丧失, 感音神经性 /
- 梅尼埃病 /
- 偏头痛 /
- 临床特征 /
- 转归
Abstract: Objective The aim of this study was to explore the clinical features, hearing prognosis and differential diagnosis of recurrent low frequency sensorineural hearing loss (RLFD).Method The clinical characteristics, clinical manifestations, audiological examination and auxiliary examination of RLFD patients were retrospectively analyzed. We summarized clinical features, draw the pure tone audiometry curves, and analyze the diagnosis of RLFD.Result Forty-seven patients (53 ears) with RLFD had a hearing review time of 1-124 months. The course of disease ranged from 3 to 320 months with an average course of 29 months. ①The incidence of tinnitus in the accompanying symptoms was 93.6%(44 cases), and the ear suffocation was 83.0%(39 cases), 38.3% (18 cases) of the patients developed vestibular symptoms during the course of the disease. ②During the observation period, 27 cases(57.4%) were diagnosed with related diseases: 7 cases(14.9%) Meniere's disease, 6 cases(12.8%) vestibular migraine, 2 cases(4.3%) with Meniere's disease and migraine, and 1 case(2.1%) with idiopathic intracranial hypotension 11 cases(23.4%) were possible cochlear migraine; ③Migraine-related RLFD had a younger onset age, more common in women; ④83.0%(44 ears)of the affected ears had stable or improved low-frequency hearing during the observation period, 17.0%(9 ears)of the affected ears experienced low-frequency hearing; ⑤18.9%(10 ears)of the affected ears had high-frequency hearing loss; ⑥RLFD had 6 types of audiological outcomes: low-frequency improvement combined with high-frequency stability; low-frequency stability combined with high-frequency stability; low frequency progress combined with high frequency stability type; low frequency improvement combined with high frequency progress type; low frequency stability combined with high frequency progress type; low frequency progress combined with high frequency progress type; ⑦Rising type hearing curve low frequency hearing prognosis is good, mountain type and descending low frequency hearing prognosis is poor.Conclusion Tinnitus and ear stuffiness are the early symptoms and the most disturbing symptoms in patients with RLFD. The mechanism of Migraine may play an important role in the pathogenesis of RLFD. The rare causes such as intracranial hypotension syndrome should not be ignored. Most of the patients with RLFD had stable or improved hearing after long-term fluctuation, but some patients with low or high frequency hearing might decline. The type of initial hearing curve was a prognostic factor. Long-term hearing follow-up is helpful for prognosis evaluation.-
Key words:
- hearing loss, sensorineural /
- Menière's disease /
- migraine /
- clinical characteristics /
- outcomes
-

-
表 1 临床特征及疾病转归总结表
临床特征及转归 例数(%) 临床特征及转归 例数(%) 性别 伴随症状 男 21(44.7) 耳鸣 44(93.6) 女 26(55.3) 耳闷 39(83.0) 诱因 声敏 15(31.9) 劳累 16(34.0) 颅鸣 3(6.4) 睡眠不足 11(23.4) 焦虑抑郁 3(6.4) 情绪波动 7(14.9) 眩晕 18(38.3) 感冒 3(6.4) 偏头痛相关 饮酒 3(6.4) 慢性头痛 15(31.9) 气温变化 2(4.3) 偏头痛家族史 7(14.9) 手术 1(2.1) 患侧颈项僵直 5(10.6) 献血 1(2.1) 畏光畏声 3(6.4) 侧别 视觉或感觉 2(4.3) 左 25(53.2) 先兆 右 16(34.0) 晕动症 6(12.8) 双耳同时 3(6.4) 相关诱因 12(25.5) 双耳交替 3(6.4) 特定药物好转 4(8.5) 首发症状 疾病转归 耳鸣 19(40.4) MD 7(14.9) 耳闷 16(34.0) CM 11(23.4) 听力下降 12(25.5) VM 6(12.8) 既往史 MD+VM 2(4.3) 高血压 2(4.3) SIH 1(2.1) 糖尿病 2(4.3) 其他 20(42.6)  下载: 导出CSV
下载: 导出CSV
表 2 听力学特征及转归
听力学特征及转归 耳数(%) 听力曲线分类 上升型 29(54.7) 山型 21(39.6) 下降型 3(5.7) 低频听力损失等级(首次/末次) 1级 12(22.6)/21(39.6) 2级 15(28.3)/14(26.4) 3级 18(34.0)/9(17.0) 4级 8(15.1)/9(17.0) 低频转归 改善 21(39.6) 稳定 23(43.4) 进展 9(17.0) 高频疗效 稳定 43(81.1) 进展 10(18.9) 听力学转归 低频改善合并高频稳定型 19(35.8) 低频稳定合并高频稳定型 18(34.0) 低频进展合并高频稳定型 6(11.3) 低频改善合并高频进展型 2(3.8) 低频稳定合并高频进展型 5(9.4) 低频进展合并高频进展型 3(5.7) 耳蜗电图或甘油试验 阳性 9(27.3) 阴性 24(72.7)
下载: 导出CSV
表 3 听力学转归相关影响因素
项目 耳数 低频改善 低频稳定 低频进展 P 年龄 36.0±10.5 36.4±10.5 36.0±10.6 0.587 性别 男 24 10(41.7) 10(41.7) 4(16.7) 0.924 女 29 11(37.9) 12(4.4) 6(20.7) BMI 21.7±3.3 22.7±5.4 25.6±3.6 0.162 眩晕 发生 20 9(45.0) 5(25.0) 6(30.0) 0.805 不发生 33 12(36.4) 18(54.5) 3(9.1) 听力随访时间 <6个月 27 8(29.6) 16(59.3) 3(11.1) 0.716 6个月~<2年 14 8(57.1) 4(28.6) 2(14.3) ≥2年 12 5(41.7) 3(25.0) 4(33.3) 病程 <1年 19 9(47.4) 9(47.4) 1(5.3) 0.215 1~<4年 17 7(41.2) 6(35.3) 4(23.5) ≥4年 17 5(29.4) 8(47.1) 4(23.5) 听力曲线 上升型 29 16(55.2) 10(34.5) 3(10.3) 0.014 山型 21 5(23.8) 12(57.1) 4(19.0) 下降型 3 0(0) 1(33.3) 2(66.6) 初测听力等级 1 12 2(16.7) 6(50.0) 4(33.3) <0.001 2 15 3(20.0) 8(53.3) 4(26.7) 3 18 10(55.6) 7(38.9) 1(5.6) 4 8 6(75.0) 2(25.0) 0(0)
下载: 导出CSV
-
[1] Lopez-Escamez JA, Carey J, Chung WH, et al. Diagnostic criteria for Meniere's disease[J]. J Vestib Res, 2015, 25(1): 1-7. doi: 10.3233/VES-150549
[2] 赖仁淙, 刘琼临. 内耳型偏头痛: 前庭性偏头痛与耳蜗性偏头痛[J]. 临床耳鼻咽喉头颈外科杂志, 2019, 33(3): 200-203. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH201903003.htm
[3] Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition(beta version)[J]. Cephalalgia, 2013, 33(9): 629-808. doi: 10.1177/0333102413485658
[4] Lempert T, Olesen J, Furman J, et al. Vestibular migraine: diagnostic criteria[J]. J Vestibular Res, 2012, 22(4): 167-172. doi: 10.3233/VES-2012-0453
[5] Schievink WI, Dodick DW, Mokri B, et al. Diagnostic criteria for headache due to spontaneous intracranial hypotension: a perspective[J]. Headache, 2011, 51(9): 1442-1444. doi: 10.1111/j.1526-4610.2011.01911.x
[6] Yoshida T, Sone M, Kitoh R, et al. Idiopathic sudden sensorineural hearing loss and acute low-tone sensorineural hearing loss: a comparison of the results of a nationwide epidemiological survey in Japan[J]. Acta Otolaryngol, 2017, 137(sup565): S38-S43. doi: 10.1080/00016489.2017.1297539
[7] Noguchi Y, Nishida H, Tokano H, et al. Comparison of acute low-tone sensorineural hearing loss versus Meniere's disease by electrocochleography[J]. Ann Otol Rhinol Laryngol, 2004, 113(3 Pt 1): 194-199.
[8] Schaaf H, Seling B, Rienhoff NK, et al. Is recurrent loss of low frequency tone perception--without vertigo--a precursor of Meniere disease?[J]. HNO, 2001, 49(7): 543-547. doi: 10.1007/s001060170079
[9] Schaaf H, Hesse G. Low frequency fluctuating hearing loss without labyrinthine vertigo--a genuine disease? A follow up study after 4 and 10 years[J]. HNO, 2007, 55(8): 630-637. doi: 10.1007/s00106-006-1495-3
[10] Chu CH, Liu CJ, Fuh JL, et al. Migraine is a risk factor for sudden sensorineural hearing loss: a nationwide population-basedstudy[J]. Cephalalgia, 2013, 33(2): 80-86. doi: 10.1177/0333102412468671
[11] Hwang JH, Tsai SJ, Liu TC, et al. Association of Tinnitus and Other Cochlear Disorders With a History of Migraines[J]. JAMA Otolaryngol Head Neck Surg, 2018, 144(8): 712-717. doi: 10.1001/jamaoto.2018.0939
[12] Radtke A, von Brevern M, Neuhauser H, et al. Vestibular migraine: long-term follow-up of clinical symptoms and vestibulo-cochlear findings[J]. Neurology, 2012, 79(15): 1607-1614. doi: 10.1212/WNL.0b013e31826e264f
[13] Moshtaghi O, Sahyouni R, Lin HW, et al. A Historical Recount: Discovering Meniere's Disease and Its Association With Migraine Headaches[J]. Otol Neurotol, 2016, 37(8): 1199-1203. doi: 10.1097/MAO.0000000000001122
[14] Lai JT, Liu TC. Proposal for a New Diagnosis for Cochlear Migraine[J]. JAMA Otolaryngol Head Neck Surg, 2018, 144(3): 185-186. doi: 10.1001/jamaoto.2017.2427
[15] Chung SJ, Kim JS, Lee MC. Syndrome of cerebral spinal fluid hypovolemia: clinical and imaging features and outcome[J]. Neurology, 2000, 55(9): 1321-1327. doi: 10.1212/WNL.55.9.1321
[16] Miller RS, Tami TA, Pensak M. Spontaneous intracranial hypotension mimicking Meniere's disease[J]. Otolaryngol Head Neck Surg, 2006, 135(4): 655-656. doi: 10.1016/j.otohns.2005.03.087
[17] Taki M, Nin F, Hasegawa T, et al. Case report: two cases of hearing impairment due to intracranial hypotension[J]. Auris Nasus Larynx, 2009, 36(3): 345-348. doi: 10.1016/j.anl.2008.05.016
[18] Nakaya M, Morita I, Horiuchi M. Recurrent hearing loss after myelography treated with epidural blood patch[J]. Auris Nasus Larynx, 2005, 32(4): 399-401. doi: 10.1016/j.anl.2005.07.013
[19] Wang DY, Wang YC, Weil D, et al. Screening mutations of OTOF gene in Chinese patients with auditory neuropathy, including a familial case of temperature-sensitive auditory neuropathy[J]. BMC Med Genet, 2010, 11: 79-79.
[20] Zhang Q, Lan L, Shi W, et al. Temperature sensitive auditory neuropathy[J]. Hear Res, 2016, 335: 53-63. doi: 10.1016/j.heares.2016.01.008
[21] Nozawa I, Imamura S, Mizukoshi A, et al. Clinical study of acute low-tone sensorineural hearing loss: survey and analysis of glycerol testand orthostatic test[J]. Ann Otol Rhinol Laryngol, 2002, 111(2): 160-164. doi: 10.1177/000348940211100209
[22] Mijovic T, Zeitouni A, Colmegna I. Autoimmune sensorineural hearing loss: the otology-rheumatology interface[J]. Rheumatology(Oxford), 2013, 52(5): 780-789. doi: 10.1093/rheumatology/ket009
[23] Marrodan M, Correale J, Alessandro L, et al. Susac Syndrome: A differential diagnosis of white matter lesions[J]. Mult Scler Relat Disord, 2017, 15: 42-46. doi: 10.1016/j.msard.2017.04.007
[24] Seale B, Ahanger S, Hari C. Subacute carbon monoxide poisoning presenting as vertigo and fluctuating low frequency hearing loss[J]. J Surg Case Rep, 2018, 2018(8): rjy205.
[25] Kanaan AA, Raad RA, Hourani RG, et al. Bilateral superior semicircular canal dehiscence in a child with sensorineural hearing loss and without vestibular symptoms[J]. Int J Pediatr Otorhinolaryngol, 2011, 75(6): 877-879. doi: 10.1016/j.ijporl.2011.03.019
-
图(1)
表(3)
计量
- 文章访问数: 1689
- PDF下载数: 1580
- 施引文献: 0