
The application of transcervical non-inflatable endoscopic posterior inferior sternocleidomastoid approach in thyroid surgery
-
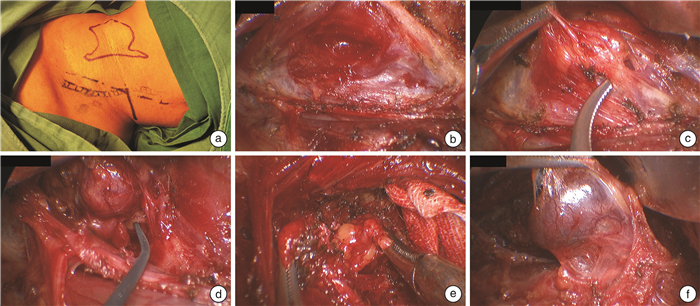
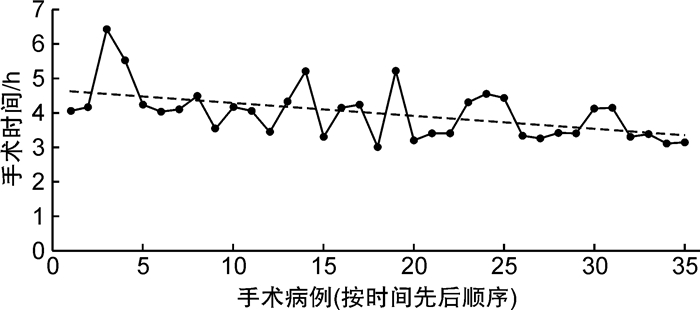
摘要: 目的 探讨无注气经颈侧腔镜胸锁乳突肌后下入路甲状腺手术的临床疗效与安全性。方法 回顾性分析2022年12月至2023年5月收治的35例行无注气经颈侧腔镜胸锁乳突肌后下入路甲状腺乳头状癌手术患者,其中男14例,女21例,平均年龄44.7岁,记录患者手术时间、出血量、术后恢复、并发症及随访情况。结果 35例患者均顺利完成手术,平均手术时间4 h 7 min,平均出血量14 mL,平均术后住院时间3.5 d,无严重并发症,术后随访未诉明显颈部不适。结论 无注气经颈侧腔镜胸锁乳突肌后下入路甲状腺手术安全性良好,患者术后恢复快,外观满意度高,颈部舒适感好。Abstract: Objective To investigate the clinical efficacy and safety of transcervical non-inflatable endoscopic thyroidectomy through the posterior inferior sternocleidomastoid approach.Methods From December 2022 to May 2023, the clinical data of 35 patients with papillary thyroid carcinoma treated by transcervical non-inflatable endoscopic surgery via posterior inferior sternocleidomastoid approach were retrospectively analyzed. There were 14 males and 21 females, with an average age of 44.7 years. The operation time, bleeding volume, postoperative recovery, complications and follow-up were recorded.Results All 35 patients successfully completed the surgery, with an average operation time of 4 hours and 7 minutes, an average bleeding volume of 14 ml, and an average postoperative hospital stay of 3.5 days. There were no serious complications and no obvious neck discomfort during postoperative follow-up.Conclusion Transcervical non-inflatable endoscopic thyroidectomy via posterior inferior sternocleidomastoid approach is safe and effective, with fast postoperative recovery, high appearance satisfaction and good neck comfort.
-

-
表 1 患者一般情况及围手术期信息
临床特征 数量/例 百分率/% 性别 男 14 40.00 女 21 60.00 年龄/岁 ≤40 14 40.00 >40~≤60 18 51.43 >60 3 8.57 肿瘤T分期 1~2 18 51.43 3~4 17 48.57 肿瘤N分期 0 18 51.43 1a 11 31.43 1b 6 17.14 手术时间/h ≤4 23 65.71 >4 12 34.29 出血量/mL ≤10 28 80.00 >10~≤30 2 5.71 >30~≤50 5 14.29 术后住院时间/d ≤4 26 74.29 >4~≤6 7 20.00 >6 2 5.71 术后并发症 无 33 94.28 乳糜漏 1 2.86 耳后麻木感 1 2.86  下载: 导出CSV
下载: 导出CSV
-
[1] Vardaxi C, Tsetsos N, Koliastasi A, et al. Swallowing disorders after thyroidectomy: a systematic review and meta-analysis[J]. Eur Arch Otorhinolaryngol, 2022, 279(9): 4213-4227. doi: 10.1007/s00405-022-07386-8
[2] Sebag F, Palazzo FF, Harding J, et al. Endoscopic lateral approach thyroid lobectomy: safe evolution from endoscopic parathyroidectom[J]. World J Surg, 2006, 30(5): 802-805. doi: 10.1007/s00268-005-0353-x
[3] 孙锦海. 经胸锁乳突肌前缘入路甲状腺切除手术治疗甲状腺肿瘤[J]. 泰山医学院学报, 2018, 39(1): 53-54. https://www.cnki.com.cn/Article/CJFDTOTAL-TSYX201801016.htm
[4] 黄海, 陈欣欣, 马宇园, 等. 经胸锁乳突肌肌间入路甲状腺癌根治手术的临床观察[J]. 现代肿瘤医学, 2020, 28(23): 4069-4072. https://www.cnki.com.cn/Article/CJFDTOTAL-SXZL202023011.htm
[5] 朱峰, 邬一军, 沈亦斌, 等. 经胸锁乳突肌肌间入路行甲状腺手术对颈前区功能保护研究[J]. 中国实用外科杂志, 2020, 40(7): 847-850. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWK202007034.htm
[6] Gohrbandt AE, Aschoff A, Gohrbandt B, et al. Changes of laryngeal mobility and symptoms following thyroid sugery: 6-month follow-up[J]. World J Surg, 2016, 40(3): 636-643. doi: 10.1007/s00268-015-3323-y
[7] Thorsen RT, Døssing H, Bonnema SJ, et al. The Impact of Post-Thyroidectomy Neck Stretching Exercises on Neck Discomfort, Pressure Symptoms, Voice and Quality of Life: A Randomized Controlled Trial[J]. World J Surg, 2022, 46(9): 2212-2222. doi: 10.1007/s00268-022-06610-0
[8] Gagner M. Endoscopic subtotal parathyroidectomy in patients with primary hyperparathyroidism[J]. Br J Surg, 1996, 83(6): 875.
[9] Hüscher CS, Chiodini S, Napolitano C, et al. Endoscopic right thyroid lobectomy[J]. Surg Endosc, 1997, 11(8): 877. doi: 10.1007/s004649900476
[10] 仇明, 丁尔迅, 江道振, 等. 颈部无瘢痕内镜甲状腺腺瘤切除术一例[J]. 中华普通外科杂志, 2002, 17(2): 127-127. https://www.cnki.com.cn/Article/CJFDTOTAL-ZHPZ200202033.htm
[11] Luna-Ortiz K, Gomez-Pedraza A, Anuwong A. Lessons learned from the transoral endoscopic thyroidectomy with vestibular approach(TOETVA)for the treatment of thyroid carcinoma[J]. Ann Surg Oncol, 2020, 27(5): 1356-1360. doi: 10.1245/s10434-019-07899-3
[12] Garstka M, Mohsin K, Ali DB, et al. Well-differentiated thyroid cancer and robotic transaxillary surgery at a North American institution[J]. J Surg Res, 2018, 228: 170-178.
[13] Byeon HK, Holsinger FC, Duvvuri U, et al. Recent progress of retroauricular robotic thyroidectomy with the new surgical robotic system[J]. Laryngoscope, 2018, 128(7): 1730-1737.
-

图(3)
表(1)
计量
- 文章访问数: 648
- PDF下载数: 113
- 施引文献: 0