
Comparison of the diagnostic value of high frequency ultrasound and ultrasound-guided fine needle aspiration biopsy in papillary thyroid microcarcinoma
-
摘要: 目的 探讨高频超声、超声引导下细针穿刺活检(US-FNAB)在甲状腺微小乳头状癌(PTMC)诊断中的应用价值,寻找PTMC更方便无创的诊断方法,减少不必要的穿刺及手术。方法 回顾性分析2020年1月到6月期间,来自河南省肿瘤医院和河南省省立医院的190例PTMC患者资料,共305个结节,其中PTMC结节198个(PTMC结节组),甲状腺良性结节(BTN)107个(BTN结节组)。通过卡方检验和Logistic回归分析结节的超声表现及颈部淋巴结能否探及等因素与PTMC的关系,并评估其诊断价值;采用Kappa一致性检验,分析高频超声、US-FNAB与术后病理结果之间的一致性;对高频超声与US-FNAB的准确率、灵敏度和特异度进行比较,通过ROC曲线计算最大曲线下面积(AUC)评估其效能。结果 卡方检验分析显示:PTMC结节组与BTN结节组的结节形态、边缘、内部回声、回声均匀度、有无钙化、纵横比、血流信号以及颈部淋巴结能否探及等超声征象的差异均有统计学意义;Logistic回归分析结果显示:形态不规则、边缘不清晰、内部低回声、结节内有钙化是PTMC的独立危险因素;经一致性检验,高频超声、US-FNAB检查与术合病理结果之间的一致性均良好,Kappa值分别为0.802、0.893(P < 0.05);每个结节均进行高频超声检查,其诊断灵敏度为95.45%,特异度为83.18%,准确率为91.15%,AUC为0.877;对305枚甲状腺结节中的189枚进行细针穿刺,其诊断灵敏度为96.03%,特异度为93.65%,准确率为95.24%,AUC为0.948。结论 内部低回声、结节内有钙化、边缘不清晰、形态不规则等超声特征对于PTMC的诊断具有很高的价值;高频超声与US-FNAB检查对PTMC的诊断价值均较高。高频超声与US-FNAB相比具有检查成本低、无创、操作简单等优点。对于没有高危因素的PTMC患者,可以通过超声积极监控疾病进展避免不必要的手术。Abstract: Objective To explore the application value of high frequency ultrasound and ultrasound-guided fine needle aspiration biopsy(US-FNAB) in the diagnosis of papillary thyroid microcarcinoma(PTMC), and to compare the characteristics and value of the two methods, so as to find a more convenient and non-invasive diagnostic method of PTMC, reduce unnecessary puncture and operation.Methods The data of 190 postoperative pathologically confirmed PTMC patients admitted to Henan Province Cancer Hospital and Henan Provincial Hospital from January to June 2020 were retrospectively analyzed, with a total of 305 nodules, including 198 PTMC nodules and 107 benign thyroid nodules(BTN). According to the postoperative pathological results, they were divided into groups, and the relationship between the ultrasound appearance of the nodules and whether the cervical lymph nodes could be explored and PTMC was analyzed by chi-square test and logistic regression, and its diagnostic value was evaluated. The Kappa consistency test was used to analyze the consistency between ultrasound, FNAB and surgical pathological diagnosis results. The accuracy, sensitivity and specificity of high-frequency ultrasound and US-FNAB were compared, and the ROC curve was used to calculate the maximum area under the curve to evaluate its effectiveness.Results The chi-square test showed that there were statistically significant differences in the morphology, margin, internal echo, echo uniformity, calcification, aspect ratio, blood flow signal, and whether the cervical lymph nodes can be detected and other ultrasound signs between the PTMC group and the BTN group. Logistic regression analysis showed that irregular shape, unclear edges, internal hypoechoic, intranodular calcification are independent risk factors for PTMC. By consistency test, the consistency between high-frequency ultrasound, US-FNAB examination and surgical pathological diagnosis was good, Kappa value was 0.802 and 0.893(P < 0.05). Each nodule was examined by high-frequency ultrasound, and the diagnostic sensitivity, specificity, accuracy and AUC were 95.45%, 83.18%, 91.15% and 0.877 respectively. US-FNAB was performed on 189 of 305 thyroid nodules, and the diagnostic sensitivity, specificity, accuracy and AUC were 96.03%, 93.65%, 95.24% and 0.948 respectively.Conclusion High frequency ultrasonic features such as internal hypoechoic, calcification in the nodules, unclear edges, and irregular morphology are of high value for the diagnosis of PTMC. Through data analysis, both high-frequency ultrasound and US-FNAB examination have high diagnostic value for PTMC. Compared with US-FNAB, high-frequency ultrasound has the advantages of low examination cost, non-invasive, simple operation and so on. For some patients with PTMC who do not have high risk factors, ultrasound can be used to actively monitor disease progression to avoid some unnecessary surgery.
-

-
表 1 PTMC结节组与BTN结节组的超声特征比较
项目 PTMC
结节组
(n=198)BTN
结节组
(n=107)χ2 P 形态 110.845 0.000 规则 41 89 不规则 157 18 边缘 125.596 0.000 清晰 37 91 不清晰 161 16 内部回声 121.871 0.000 低回声 173 26 其他 25 81 回声均匀度 6.129 0.013 均匀 71 54 不均匀 127 53 有无钙化 55.107 0.000 有 127 21 无 71 86 血流信号 5.714 0.017 有 65 50 无 133 57 纵横比 21.498 0.000 >1 46 3 < 1 152 104 颈部淋巴结情况 12.612 0.000 可探及 74 19 未探及 124 88  下载: 导出CSV
下载: 导出CSV
表 2 Logistic回归分析各因素与PTMC的关联程度
变量 偏回归系数 Wald P OR CI 下限 上限 形态 1.272 9.235 0.002 3.567 1.571 8.099 边缘 1.895 18.595 0.000 6.652 2.811 15.740 内部低回声 1.956 22.837 0.000 7.073 3.171 15.777 有无钙化 2.260 17.326 0.000 9.584 3.306 27.779 血流信号 0.032 0.006 0.938 1.033 0.461 2.311 回声均匀度 1.551 7.250 0.107 4.715 1.525 14.577 纵横比 0.910 1.644 0.200 2.484 0.618 9.983 颈部淋巴结情况 0.146 0.085 0.771 1.157 0.434 3.087
下载: 导出CSV
表 3 高频超声结果与术后病理对比
确诊方式 病理结果 合计 PTMC(+) 良性(-) 超声检查 恶性(+) 189 18 207 良性(-) 9 89 98 合计 198 107 305
下载: 导出CSV
表 4 US-FNAB结果与术后病理对比
确诊方式 病理结果 合计 PTMC(+) 良性(-) US-FNAB检查 恶性(+) 121 4 125 良性(-) 5 59 64 合计 126 63 189
下载: 导出CSV
表 5 US-FNAB检查结果与超声检查结果准确度对比
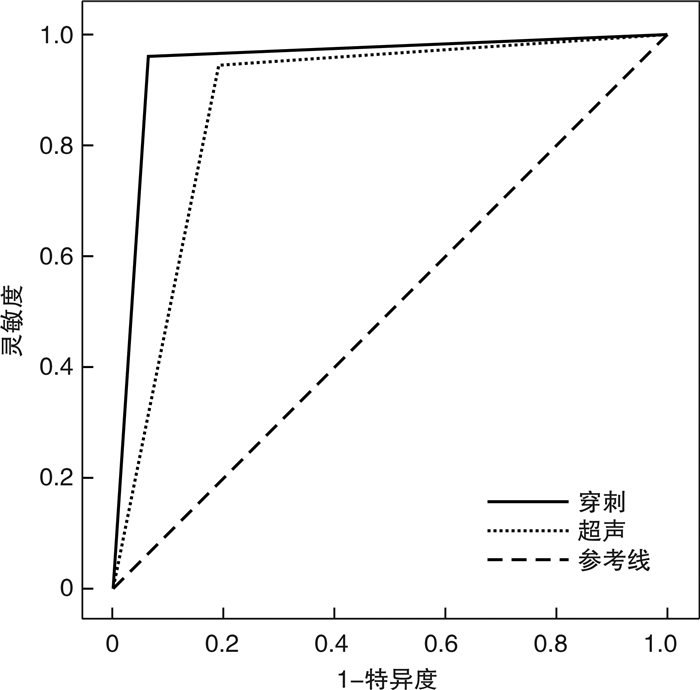
检查方法 灵敏度/% 特异度/% 准确率/% AUC 超声检查 95.45 83.18 91.15 0.877 US-FNAB检查 96.03 93.65 95.24 0.948
下载: 导出CSV
-
[1] Xu JM, Xu HX, Li XL, et al. A Risk Model for Predicting Central Lymph Node Metastasis of Papillary Thyroid Microcarcinoma Including Conventional Ultrasound and Acoustic Radiation Force Impulse Elastography[J]. Medicine(Baltimore), 2016, 95(3): e2558.
[2] 孙可敏, 何秀丽, 郭玲玲. 甲状腺微小乳头状癌临床及超声特征与中央区淋巴结转移的危险因素[J]. 临床耳鼻咽喉头颈外科杂志, 2021, 35(3): 260-263. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH202103016.htm
[3] So YK, Son YI, Hong SD, et al. Subclinical lymph node metastasis in papillary thyroid microcarcinoma: a study of 551 resections[J]. Surgery, 2010, 148(3): 526-531. doi: 10.1016/j.surg.2010.01.003
[4] Varsavsky M, Cortés Berdonces M, Alonso G, et al. [Metastatic adenopathy from a thyroid microcarcinoma: final diagnosis of a presumed paraganglioma][J]. Endocrinol Nutr, 2011, 58(3): 143-144. doi: 10.1016/j.endonu.2010.10.009
[5] Abooshahab R, Gholami M, Sanoie M, et al. Advances in metabolomics of thyroid cancer diagnosis and metabolic regulation[J]. Endocrine, 2019, 65(1): 1-14. doi: 10.1007/s12020-019-01904-1
[6] 赵美丽, 杨炜, 李金凤, 等. 超声引导下细针穿刺细胞学检测不同大小可疑甲状腺癌结节的阳性率及准确率[J]. 南方医科大学学报, 2020, 40(5): 693-697. https://www.cnki.com.cn/Article/CJFDTOTAL-DYJD202005013.htm
[7] Haugen BR, Alexander EK, Bible KC, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer[J]. Thyroid, 2015, 123(1): 1-133.
[8] 毕腾云, 白文坤, 胡兵. 甲状腺超声钙化形态与甲状腺癌的关系[J]. 中国超声医学杂志, 2016, 32(6): 481-483. doi: 10.3969/j.issn.1002-0101.2016.06.001
[9] Kwak JY, Han KH, Yoon JH, et al. Thyroid imaging reporting and data system for US features of nodules: a step in establishing better stratification of cancer risk[J]. Radiology, 2011, 260(3): 892-899. doi: 10.1148/radiol.11110206
[10] Cibas ES, Ali SZ. The 2017 Bethesda System for Reporting Thyroid Cytopathology[J]. Thyroid, 2017, 27(11): 1341-1346. doi: 10.1089/thy.2017.0500
[11] Liu X, Sun J, Fang W, et al. Current Iodine Nutrition Status and Morbidity of Thyroid Nodules in Mainland China in the Past 20 Years[J]. Biol Trace Elem Res, 2021.
[12] 安祥, 余丹, 李兵. 预防性中央区淋巴结清扫对甲状腺微小乳头状癌患者预后影响的Meta分析[J]. 临床耳鼻咽喉头颈外科杂志, 2019, 33(2): 138-142. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH201902011.htm
[13] 中华人民共和国国家卫生健康委员会. 甲状腺癌诊疗规范(2018年版)[J]. 中华普通外科学文献(电子版), 2019, 13(1): 1-15. doi: 10.3877/cma.j.issn.1674-0793.2019.01.001
[14] Ito Y, Miyauchi A, Kihara M, et al. Patient age is significantly related to the progression of papillary microcarcinoma of the thyroid under observation[J]. Thyroid, 2014, 24(1): 27-34. doi: 10.1089/thy.2013.0367
[15] 周明炀, 费小春, 詹维伟, 等. 甲状腺微小乳头状癌常见超声表现的病理学基础[J]. 中华医学超声杂志(电子版), 2014, 11(5): 383-387. doi: 10.3877/cma.j.issn.1672-6448.2014.05.006
[16] Kim BK, Choi YS, Kwon HJ, et al. Relationship between patterns of calcification in thyroid nodules and histopathologic findings[J]. Endocr J, 2013, 60(2): 155-160. doi: 10.1507/endocrj.EJ12-0294
[17] Alexander LF, Patel NJ, Caserta MP, et al. Thyroid Ultrasound: Diffuse and Nodular Disease[J]. Radiol Clin North Am, 2020, 58(6): 1041-1057. doi: 10.1016/j.rcl.2020.07.003
[18] Wang CC, Friedman L, Kennedy GC, et al. A large multicenter correlation study of thyroid nodule cytopathology and histopathology[J]. Thyroid, 2011, 21(3): 243-251. doi: 10.1089/thy.2010.0243
[19] Sung JY, Na DG, Kim KS, et al. Diagnostic accuracy of fine-needle aspiration versus core-needle biopsy for the diagnosis of thyroid malignancy in a clinical cohort[J]. Eur Radiol, 2012, 22(7): 1564-1572. doi: 10.1007/s00330-012-2405-6
[20] 雍慧娟, 徐书杭, 刘超. 甲状腺微小乳头状癌的临床诊治[J]. 中华内分泌代谢杂志, 2018, 34(4): 353-358. doi: 10.3760/cma.j.issn.1000-6699.2018.04.017
-
图(1)
表(5)
计量
- 文章访问数: 636
- PDF下载数: 178
- 施引文献: 0