
Analysis of esophageal manometry results and the inflection point of age in 41 volunteers without laryngopharyngeal symptoms
-
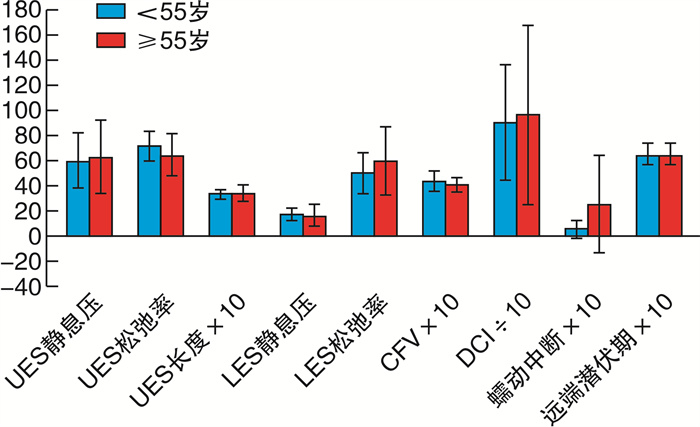
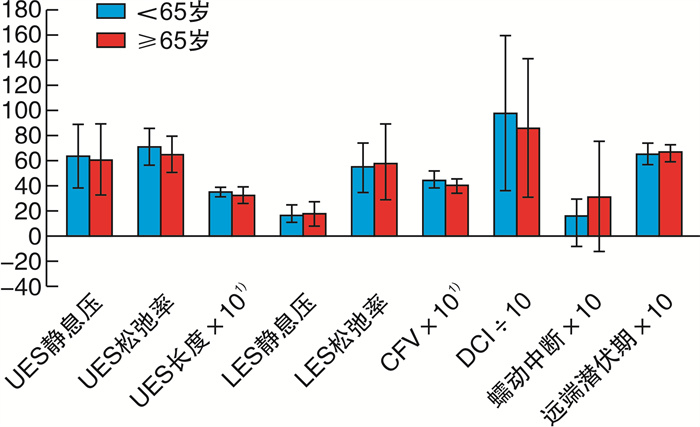
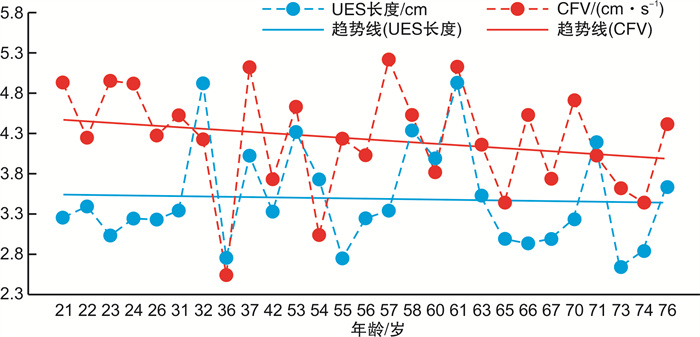
摘要: 目的 探讨不同年龄食管压力的差异, 同时分析食管动力生理性退化的可能年龄拐点, 进一步评估随着年龄增长食管动力学的退化是否是咽喉反流性疾病(LPRD)发生的唯一危险因素。方法 对41例无咽喉症状的志愿者进行固态高分辨率食管测压, 将其结果与芝加哥标准进行比对, 并比较预设年龄拐点组间人群的食管测压结果。结果 大部分志愿者的食管测压结果均符合芝加哥标准。其中, 以55岁为年龄拐点分组, 两组间各项食管动力学数据分析结果均P>0.05;以65岁为年龄拐点分组, 两组间食管上括约肌长度及收缩前沿速度的差异有统计学意义(P = 0.021及0.046)。结论 随着年龄的增长, 无咽喉反流症状人群中食管动力会发生一定程度的退化, 这种变化在65岁后较为明显, 但仍在正常范围内。食管动力学的退变不是LPRD发生的唯一危险因素。Abstract: Objective This study aimed to explore the differences in esophageal pressure at different ages, and to analyze the possible age inflection points of the physiological degeneration of esophageal motility, and to further evaluate whether the degeneration of esophageal kinetics with age is the only risk factor for the occurrence of throat reflux disease (LPRD).Methods A solid-state high-resolution esophageal pressure measurement was performed on 41 volunteers without throat symptoms. The Chicago classification data were compared with the manometry results of all volunteers. In addition, the esophageal manometry results were compared among groups with pre-set age inflection point.Results Most of the volunteers' esophageal pressure measurements were in line with Chicago standards. When the inflection point of age was 55 years, no significant difference was found between the two groups. However, when the inflection point of age was 65 years, a significant difference in the length of the upper esophageal sphincter and the contractile front velocity was found between the two groups(P = 0.021 and 0.046 respectively).Conclusion Esophageal dynamics was weakened with increasing age in the volunteers without laryngopharyngeal symptoms, which was more obvious after the age of 65, but still within the normal range. The degeneration of esophageal motility is not the only risk factor for LPRD.
-

-
表 1 41例无咽喉症状志愿者食管动力结果与正常值的比较
观察指标 志愿者 正常者 UES静息压/mmHg 61.63±25.03 40~140 UES长度/cm 3.34±0.49 3~4 LES静息压/mmHg 16.61±7.12 10~30 CFV/(cm·s-1) 4.21±0.72 < 9 DCI/(mmHg·s-1·cm-1) 934.41±585.93 450~8000 蠕动中断/cm 1.54±2.81 < 5 DL/s 6.44±0.81 ≥4.5  下载: 导出CSV
下载: 导出CSV
-
[1] 李真, 李延青. 2013国际胃食管反流病诊断和管理指南解读[J]. 中国医学前沿杂志(电子版), 2013, 5(5): 57-63. doi: 10.3969/j.issn.1674-7372.2013.05.021
[2] Salihefendic N, Zildzic M, Cabric E. Laryngopharyngeal Reflux Disease-LPRD[J]. Med Arch, 2017, 71(3): 215-218. doi: 10.5455/medarh.2017.71.215-218
[3] Ceccatelli P, Mariottini M, Agnolucci A, et al. Acid exposure of proximal esophagus in healthy subjects[J]. Minerva Gastroenterol Dietol, 1998, 44(3): 129-134.
[4] 欧阳天斌. 咽喉反流疾病发病机制及诊断的相关进展[J]. 山东大学耳鼻喉眼学报, 2010, 24(5): 48-51. https://www.cnki.com.cn/Article/CJFDTOTAL-SDYU201005017.htm
[5] 朱宝宇, 宋德锋, 施春雨, 等. 胃食管反流病发病机制研究进展[J]. 中国实验诊断学, 2015, 5(2): 344-346. https://www.cnki.com.cn/Article/CJFDTOTAL-ZSZD201502068.htm
[6] 张正. 胃食管反流病[M]//叶任高. 内科学. 5版. 北京: 人民卫生出版社, 2000: 384-386.
[7] Halum SL, Postma GN, Johnston C, et al. Patients with isolated laryngopharyngeal reflux are not obese[J]. Larynoseope, 2005, 115(6): 1042-1045.
[8] Mohammed I, Cherkas LF, Riley SA, et al. Genetic influences in gastro-oesophageal reflux disease: a twin study[J]. Gut, 2003, 52(8): 1085-1089. doi: 10.1136/gut.52.8.1085
[9] Sadowski DC, Broenink L. High-resolution esophageal manometry: a time motion study[J]. Can J Gastroenterol, 2008, 22(4): 365-368. doi: 10.1155/2008/737062
[10] 李莉, 彭丽华. 高分辨率测压法在食管动力检测中的临床应用[J]. 胃肠病学和肝病学杂志, 2011, 20(3): 279-282. doi: 10.3969/j.issn.1006-5709.2011.03.025
[11] Omari TI, Barnett CP, Benninga MA, et al. Mechanisms of gastro-oesophageal reflux in preterm and term infants with reflux disease[J]. Gut, 2002, 51(4): 475-479. doi: 10.1136/gut.51.4.475
[12] Szczesniak MM, Fuentealbs SE, Cook IJ. Acid sensitization of esophageal mucosal afferents: implication for symptom perception in patients across the gastroesophageal reflux disease spectrum[J]. Clin J Pain, 2013, 29(1): 70-77. doi: 10.1097/AJP.0b013e3182478826
[13] Kamani T, Penney S, Mitra I, et al. The prevalence of larynopharyngeal refluxin the English population[J]. Eur Arch Otorhinolaryngol, 2012, 269(10): 2219-2225. doi: 10.1007/s00405-012-2028-1
[14] 姚泰, 朱进霞. 生理学[M]. 2版. 北京: 人民卫生出版社, 2010: 266-266.
[15] Singh S, Hamdy S. The upper oesophageal sphincter[J]. Neurogastroenterol Motil, 2005, 17 Suppl 1: 3-12.
[16] Sivarao DV, Goyal RK. Functional anatomy and physiology of the upper esophageal sphincter[J]. Am J Med, 2000, 108 Suppl 4a: 27S-37S.
[17] 涂丽莉, 徐胜春, 刘业海, 等. 食管上括约肌的应用解剖及临床意义[J]. 安徽医科大学学报, 2006, 41(5): 508-510. doi: 10.3969/j.issn.1000-1492.2006.05.008
[18] Medda BK, Lang IM, Dodds WJ, et al. Correlation of electrical and contractile activities of the cricopharyngeus muscle in the cat[J]. Am J Physiol, 1997, 273(2 Pt 1): G470-479.
[19] 徐甜甜, 舒继红. 咽喉反流性疾病的发病机制及诊疗进展[J]. 国际耳鼻咽喉头颈外科杂志, 2016, 40(5): 286-290. doi: 10.3760/cma.j.issn.1673-4106.2016.05.007
[20] Martinucci I, De Bortoli N, G iacchino M, et al. Esophageal motility abnormalities in gastroesophageal reflux disease[J]. World Gastrointest Pharmcaol Ther, 2014, 5(2): 86-96. doi: 10.4292/wjgpt.v5.i2.86
[21] 裴艳香, 尚占民, 郝建宇. 年龄与胃食管反流病的关系[J]. 世界华人消化杂志, 2013, 21(10): 904-907. https://www.cnki.com.cn/Article/CJFDTOTAL-XXHB201310017.htm
[22] Pilotto A, Franceschi M, Leandro G, et al. Clinical features of reflux esophagitis in older people: a study of 840 consecutive patients[J]. J Am Geriatr Soc, 2006, 54(10): 1537-1542. doi: 10.1111/j.1532-5415.2006.00899.x
[23] 吴欢, 柯美云. 改变不良生活方式和饮食习惯在胃食管反流病治疗中的作用[J]. 胃肠病学, 2009, 14(8): 449-452. https://www.cnki.com.cn/Article/CJFDTOTAL-WIEC200908004.htm
-
图(4)
表(1)
计量
- 文章访问数: 1644
- PDF下载数: 558
- 施引文献: 0