
Application of iodine staining in transoral laser microsurgery for early glottic carcinoma
-
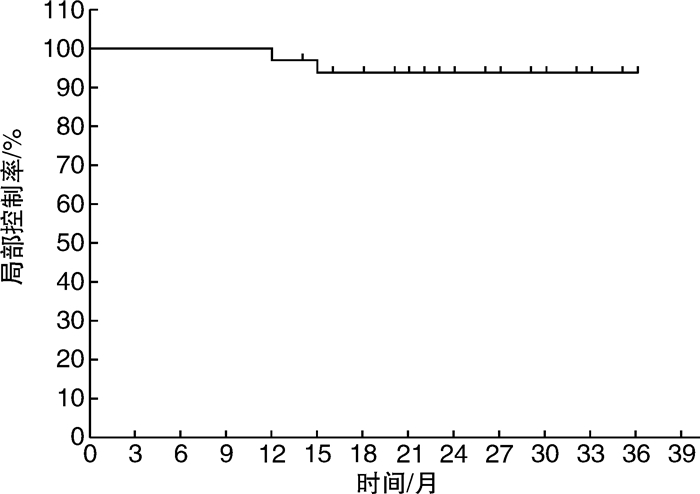
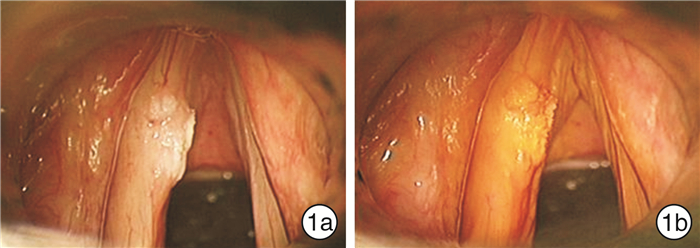
摘要: 目的 探讨碘染色在早期声门型喉癌经口激光显微手术中切缘判定的应用价值。方法 2016-01-2017-12纳入研究的早期声门型喉癌(Tis-T2)患者35例,全身麻醉后用1.5%Lugol碘溶液涂布声带3遍,手术显微镜下观察喉腔着色情况,以辅助判定病变范围。以CO2激光整块切除病变。评价并发症发生率、病灶完整切除率、复发率。结果 35例患者在经口激光显微手术中使用了碘染色辅助判断病变范围。无一例患者发生并发症。术后病理结果显示病灶的完整切除率为88.6%。Tis和T1a无局部复发病例,T1b局部复发率为12.5%,T2局部复发率为16.7%,总体局部复发率为5.7%。结论 在早期声门型喉癌经口激光显微手术中应用碘染色有助于提高完整切除率和局部控制率,是一种可靠、简单、成本低廉的方法,值得临床推广应用。Abstract: Objective To evaluate the value of iodine staining in the margin determination in transoral laser microsurgery for early glottic carcinoma.Method 35 patients with early glottic laryngeal cancer(Tis-T2) were enrolled in this study from January 2016 to December 2017.All patients were applied with 1.5% Lugol iodine solution to vocal cords for 3 times after general anesthesia, and the coloration of the laryngeal cavity was observed under the operation microscope to determine the lesion margins.The lesions were excised completely with CO2 laser.The complications, complete resection rate and recurrence rate were evaluated.Result In all patients, iodine staining was used to assist in determining the lesion range during transoral laser microsurgery.None of the patients had complications.Postoperative pathological results showed that the complete resection rate was 88.6%.There were no local recurrence cases in Tis and T1a, while local recurrence rate was 12.5% in T1b and 16.7% in T2, respectively.The overall local recurrence rate was 5.7%.Conclusion The application of iodine staining in transoral laser microsurgery for early glottic carcinoma may help improve the complete resection rate and local control rate.It is a reliable, simple and low-cost method, worthy of further clinical application.
-
Key words:
- laryngeal neoplasms /
- glottis /
- transoral laser microsurgery /
- iodine staining
-

-
表 1 不同T分期的切缘和复发情况
例 T分期 表面切缘 底切缘 复发 阳性 邻近 阴性 阳性 邻近 阴性 Tis 0 0 0 0 0 0 0 T1a 0 2 0 0 1 0 0 T1b 0 0 0 1 0 0 1 T2 0 1 0 0 0 0 1 合计 0 3 0 1 1 0 2  下载: 导出CSV
下载: 导出CSV
-
[1] Steuer CE, El-Deiry M, Parks JR, et al. An update on larynx cancer[J]. CA Cancer J Clin, 2017, 67(1): 31-50. doi: 10.3322/caac.21386
[2] Hartl DM, Brasnu DF. Contemporary Surgical Management of Early Glottic Cancer[J]. Otolaryngol Clin North Am, 2015, 48(4): 611-625. doi: 10.1016/j.otc.2015.04.007
[3] Low TH, Yeh D, Zhang T, et al. Evaluating organ preservation outcome as treatment endpoint for T1aN0 glottic cancer[J]. Laryngoscope, 2017, 127(6): 1322-1327. doi: 10.1002/lary.26317
[4] Piazza C, Paderno A, Grazioli P, et al. Laryngeal exposure and margin status in glottic cancer treated by transoral laser microsurgery[J]. Laryngoscope, 2018, 128(5): 1146-1151. doi: 10.1002/lary.26861
[5] Garofolo S, Piazza C, Del Bon F, et al. Intraoperative narrow band imaging better delineates superficial resection margins during transoral laser microsurgery for early glottic cancer[J]. Ann Otol Rhinol Laryngol, 2015, 124(4): 294-298. doi: 10.1177/0003489414556082
[6] Elimairi I, Altay MA, Abdoun O, et al. Clinical relevance of the utilization of vital Lugol's iodine staining in detection and diagnosis of oral cancer and dysplasia[J]. Clin Oral Investig, 2017, 21(2): 589-595. doi: 10.1007/s00784-016-1925-x
[7] Petruzzi M, Lucchese A, Baldoni E, et al. Use of Lugol's iodine in oral cancer diagnosis: an overview[J]. Oral Oncol, 2010, 46(11): 811-813. doi: 10.1016/j.oraloncology.2010.07.013
[8] Dawsey SM, Fleischer DE, Wang GQ, et al. Mucosal iodine staining improves endoscopic visualization of squamous dysplasia and squamous cell carcinoma of the esophagus in Linxian, China[J]. Cancer, 1998, 83(2): 220-231. doi: 10.1002/(SICI)1097-0142(19980715)83:2<220::AID-CNCR4>3.0.CO;2-U
[9] Fagundes RB, de Barros SG, Putten AC, et al. Occult dysplasia is disclosed by Lugol chromoendoscopy in alcoholics at high risk for squamous cell carcinoma of the esophagus[J]. Endoscopy, 1999, 31(4): 281-285. doi: 10.1055/s-1999-122
[10] Kuwabara H, Abe S, Nonaka S, et al. Clinical feasibility of endoscopic submucosal dissection with minimum lateral margin of superficial esophageal squamous cell carcinoma[J]. Endosc Int Open, 2019, 7(4): E396-E402. doi: 10.1055/a-0838-5064
[11] 文武林, 马瑞霞, 杨志超, 等. 电子喉镜下喉部碘溶液染色诊断早期喉癌的临床应用研究[J]. 临床耳鼻咽喉头颈外科杂志, 2016, 30(11): 873-877. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH201611009.htm
[12] Sjogren EV. Transoral Laser Microsurgery in Early Glottic Lesions[J]. Curr Otorhinolaryngol Rep, 2017, 5(1): 56-68. doi: 10.1007/s40136-017-0148-2
[13] Wilkie MD, Lightbody KA, Lythgoe D, et al. Transoral laser microsurgery for early and moderately advanced laryngeal cancers: outcomes from a single centralised United Kingdom centre[J]. Eur Arch Otorhinolaryngol, 2015, 272(3): 695-704. doi: 10.1007/s00405-014-3011-9
[14] To K, Qureishi A, Mortimore S, et al. The role of primary transoral laser microsurgery in laryngeal cancer: a retrospective study[J]. Clin Otolaryngol, 2015, 40(5): 449-455. doi: 10.1111/coa.12397
[15] Breda E, Catarino R, Monteiro E. Transoral laser microsurgery for laryngeal carcinoma: Survival analysis in a hospital-based population[J]. Head Neck, 2015, 37(8): 1181-1186. doi: 10.1002/hed.23728
[16] Bertino G, Degiorgi G, Tinelli C, et al. CO(2) laser cordectomy for T1-T2 glottic cancer: oncological and functional long-term results[J]. Eur Arch Otorhinolaryngol, 2015, 272(9): 2389-2395. doi: 10.1007/s00405-015-3629-2
[17] Roedel RM, Matthias C, Wolff HA, et al. Repeated transoral laser microsurgery for early and advanced recurrence of early glottic cancer after primary laser resection[J]. Auris Nasus Larynx, 2010, 37(3): 340-346. doi: 10.1016/j.anl.2009.07.004
[18] Huang J, Yu Z, Fang J, et al. Salvage transoral laser microsurgery for early recurrent glottic carcinoma after primary laser treatment[J]. Acta Otolaryngol, 2013, 133(5): 531-537. doi: 10.3109/00016489.2012.734929
[19] Nasef HO, Thabet H, Piazza C, et al. Prospective analysis of functional swallowing outcome after resection of T2 glottic carcinoma using transoral laser surgery and external vertical hemilaryngectomy[J]. Eur Arch Otorhinolaryngol, 2016, 273(8): 2133-2140. doi: 10.1007/s00405-016-4065-7
[20] Peretti G, Piazza C, Del Bon F, et al. Function preservation using transoral laser surgery for T2-T3 glottic cancer: oncologic, vocal, and swallowing outcomes[J]. Eur Arch Otorhinolaryngol, 2013, 270(8): 2275-2281. doi: 10.1007/s00405-013-2461-9
[21] Hughes OR, Stone N, Kraft M, et al. Optical and molecular techniques to identify tumor margins within the larynx[J]. Head Neck, 2010, 32(11): 1544-1553. doi: 10.1002/hed.21321
[22] Piazza C, Cocco D, De Benedetto L, et al. Narrow band imaging and high definition television in the assessment of laryngeal cancer: a prospective study on 279 patients[J]. Eur Arch Otorhinolaryngol, 2010, 267(3): 409-414. doi: 10.1007/s00405-009-1121-6
[23] Bertino G, Cacciola S, Fernandes WB Jr, et al. Effectiveness of narrow band imaging in the detection of premalignant and malignant lesions of the larynx: validation of a new endoscopic clinical classification[J]. Head Neck, 2015, 37(2): 215-222. doi: 10.1002/hed.23582
[24] Kraft M, Fostiropoulos K, Gurtler N, et al. Value of narrow band imaging in the early diagnosis of laryngeal cancer[J]. Head Neck, 2016, 38(1): 15-20. doi: 10.1002/hed.23838
[25] El-Shalakany AH, Saeed MM, Abdel-Aal MR, et al. Direct visual inspection of the cervix with Lugol iodine for the detection of premalignant lesions[J]. J Low Genit Tract Dis, 2008, 12(3): 193-198. doi: 10.1097/LGT.0b013e31815f527c
[26] Fennerty MB. Tissue staining[J]. Gastrointest Endosc Clin N Am, 1994, 4(2): 297-311. doi: 10.1016/S1052-5157(18)30506-3
[27] Silverman S Jr, Barbosa J, Kearns G. Ultrastructural and histochemical localization of glycogen in human normal and hyperkeratotic oral epithelium[J]. Arch Oral Biol, 1971, 16(4): 423-434. doi: 10.1016/0003-9969(71)90166-X
[28] Ashrafian H. Cancer's sweet tooth: the Janus effect of glucose metabolism in tumorigenesis[J]. Lancet, 2006, 367(9510): 618-621. doi: 10.1016/S0140-6736(06)68228-7
-
图(2)
表(1)
计量
- 文章访问数: 845
- PDF下载数: 210
- 施引文献: 0